Original Article 1, Issue 3.4
Does CPAP Pressure Predict Treatment Outcome with Oral Appliances?
http://dx.doi.org/10.15331/jdsm.6248
Leslie C. Dort, DDS1 ; Nicole Savard, RT2 ; Erika Dort, MSc3 ; Malcolm Dort, BSc2 ; Joseph Dort, MD1
1 University of Calgary, Calgary, AB, Canada; 2Calgary, AB, Canada; 3University of Victoria, BC, Canada
ABSTRACT
Study Objectives:
Oral appliance (OA) therapy can be an effective treatment for obstructive sleep apnea (OSA); however, there is significant uncertainty in predicting the outcome of OA therapy for an individual. Two previous studies have investigated the association between effective continuous positive airway pressure (CPAP) and OA therapy outcomes in controlled clinical research settings. The aim of this study was to examine the relationship between effective CPAP pressure and OA therapy outcome in a clinical setting.
Methods:
This retrospective study investigated the association between the response to OA therapy and effective CPAP pressure utilizing the same 3 criteria for response as previous studies. Effective CPAP pressure was taken from either a trial or ongoing use of CPAP. Subjects were fitted with a custom, adjustable mandibular advancement device (OA) and were sleep tested at home after acclimatization to wearing the OA and mandibular position was adjusted to maximize symptomatic response.
Results:
One hundred twenty subjects were included. Subjects were predominately male (85%), middle-aged (53.0 ± 9.9 y), overweight (BMI 30.3 ± 5.0 kg/m2 ) individuals with moderate OSA (RDI 25.6 ± 18.7 events/h). Complete response to OA therapy in the 120 subjects ranged from 34% to 65% depending on response criteria. CPAP pressure was less in those responding to OA therapy (RDI < 5 events/h) 89.0 ± 1.8 cm H2O versus non-responders 10.1 ± 2.5 cm H2O, p < 0.01 with area under the ROC curve of 0.64 (95% CI 0.54–0.74), p < 0.02. A CPAP pressure ≤ 9 cm H2O was optimal for predicting response.
Conclusions:
Effective CPAP pressure is weakly associated with OA treatment outcome.
Keywords:
oral appliance therapy, therapeutic outcomes, CPAP therapy pressure
Citation:
Dort LC, Savard N, Dort E, Dort M, Dort J. Does CPAP pressure predict treatment outcome with oral appliances? Journal of Dental Sleep Medicine 2016;3(4):113–117..
INTRODUCTION
Obstructive sleep apnea (OSA) is a common condition characterized by repetitive narrowing and collapse of the pharynx during sleep. Pharyngeal narrowing creates substantial reduction in airflow (hypopnea), and pharyngeal collapse results in cessation of airflow (apnea). These interruptions in breathing disrupt blood gases leading to hypercapnic and hypoxic conditions.1 OSA is associated with significant comorbidities including cardiovascular disease, stroke, and early mortality.2 The quality of life impact of OSA includes excessive daytime fatigue, unrefreshing sleep, impaired cognition, and increased risk of motor vehicle accidents.3,4
Mild to moderate OSA is present in up to 17% of adults, and severe OSA occurs in at least 6% of adults.5 Obesity, age, and sex are important risk factors for OSA, and the prevalence of OSA is expected to rise with the rising prevalence of obesity.5,6
The recommended treatments for OSA are continuous positive airway pressure (CPAP) and oral appliances (OA).7 Optimal CPAP pressure is the pressure that will maintain an open airway in all sleep position and sleep stages.8 While CPAP has been shown to be effective for those who choose to use it, adherence to treatment is poor. When adherence is defined as a minimum of 4 hours use a night, 46% to 83% of subjects are non-adherent to CPAP.9 OAs are the first choice alternative to CPAP. In randomized trials comparing CPAP to OAs, patients generally preferred OAs: however, OAs are less effective than CPAP in reducing the apnea-hypopnea index (AHI).10–13 There is growing evidence that OAs improve both the symptoms of OSA13–15 and the physiologic impacts such as cardiac function and hypertension.15,16–18 The application of OAs in the treatment of OSA is restricted by the limited reliability of predicting outcome with their use.19–21 As OAs must be custom made for each individual patient, a trial period or rental period is not possible as it is with a CPAP machine. There is therefore a need to predict which patients will have a favorable treatment outcome with OAs. As many patients have a period of CPAP prior to therapy with an OA, their optimal or effective CPAP pressure is known. Effective CPAP pressure is known to increase with both severity of OSA and obesity, and the effectiveness of OAs is less predictable with severity of OSA and obesity.22,23 Two recent studies have investigated the association between CPAP pressure and OA outcome. Tsuikil investigated effective CPAP pressure as a predictor of OA outcome in 35 non-obese Japanese males with severe OSA who had been using of CPAP for an average of 9 months. In this group a CPAP pressure > 10.5 cm H2O was predictive of poor response to OA therapy.24 Sutherland explored effective CPAP pressure as a predictor of OA outcome in a cohort of 78 Australian, predominantly male, overweight subjects who were treated with both OAs and CPAP in a randomized crossover trial. A CPAP pressure of 13 cm H2O was found to be predictive of OA non-response.25 The above studies each used a single but different OA design.
A typical dental sleep medicine clinical practice will include patients treated with a variety of oral appliance designs. It is common for those seeking oral appliance therapy to have had a CPAP trial but less common for them to be long-term CPAP users. The objective of this study is to explore the generalizability of the association between optimal CPAP pressure and the outcome of OA therapy in clinical practice where patients are treated with a variety of OA designs and have had at least a CPAP trial.
METHODS
The protocol was approved by the Conjoint Health Research Ethics Board of the Faculty of Medicine at the University of Calgary. This retrospective study included all patients in the private clinical practice of one of the authors (LD) from 2004 until 2012 who had a posttreatment sleep test determining response to oral appliance (OA) therapy and who also had a CPAP trial or who were on long-term CPAP therapy. Patients were excluded if they had upper airway surgery for OSA after baseline sleep testing.
Patients were referred to the clinic for evaluation for oral appliance therapy. Patients were treatment naïve, had failed CPAP, had unsuccessful surgery, or wished to use an oral appliance as alternative therapy when not able to use CPAP.
Oral Appliance Therapy Protocol
Patients referred for OA therapy underwent examination and consultation to determine appropriateness for therapy. Patients were excluded if they had too few teeth to retain an appliance, extensive periodontal disease, acute temporo-mandibular joint dysfunction, were in active orthodontic treatment, or had completed orthodontic treatment less than two years previously.
Patients who were appropriate for OA therapy, as limited by the exclusion criteria, and chose to proceed were fitted with one of a number of possible OA designs all with previously established clinical efficacy and FDA 510K acceptance.11–13,26–29 Adaptation and titration of the OA involved 5–8 clinic visits over a period of 3–5 months. When subjective symptoms had improved or maximum tolerable mandibular advancement was achieved, a follow-up sleep test was conducted. If the first follow-up sleep test indicated suboptimal effect, further mandibular advancement of the device and further testing was conducted until maximum effectiveness was achieved. Patients were then seen for routine follow-up in 6 months and yearly thereafter.
CPAP Pressure
Patients had been prescribed a variety of commercially available CPAP machines employing either fixed or auto-titrating capabilities. The effective CPAP pressure was either the fixed pressure at which the machine was set or the 90% pressure in the case of most auto-titrating machines. In the case of autotitrating machines, the 90% pressure is the setting the machine was at or below 90% of the time it was in use.
Sleep Testing
The baseline and outcome sleep testing was conducted with home sleep monitors, type 3 and 4, depending on the monitor used by the referring physician. The respiratory disturbance index (RDI) used is therefore the number of apneas and hypopneas per hour of recording.
Treatment Response Definitions
We used the same three definitions of success used in previous studies to facilitate comparisons. The first was a reduction in RDI with the OA to ≤ 5 events/h and a decrease in RDI ≥ 50%. The second was a reduction in RDI to ≤ 10 events/h and a decrease in RDI ≥ 50%. The third was a reduction in RDI ≥ 50%.Statistical Analysis
Statistical analyses were conducted with statistical software (Stata13.1 Statacorp). Independent t-tests and χ2 tests were used for continuous and categorical variables, respectively, to compare values before and after OA therapy. Logistic regression was used to identify the best models to predict OAT outcome.RESULTS
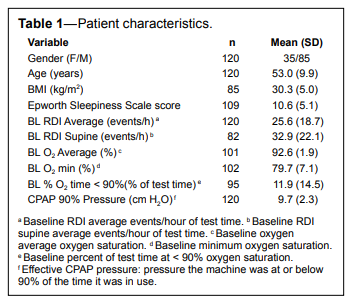
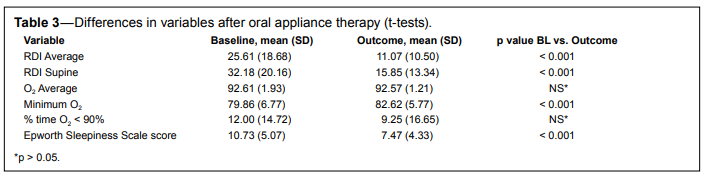
The subjects were predominantly male, middle-aged, and overweight individuals with moderate OSA (Table 1). They reported mild sleepiness and the mean CPAP pressure was 9.7 ± 2.3 (± SD) with a range of 5–18 cm H2O. The CPAP machines were primarily auto-titrating and manufactured by ResMed (Table 2). The mean outcome RDI with an OA was 60% less than the mean baseline RDI. The outcome variables significantly changed compared to baseline were: Average RDI, Supine RDI, minimum O2, and ESS (Table 3).
Table 1Patient characteristics. |
{kind=link}
Table 2CPAP delivery methods. |
{kind=link}
Table 3Differences in variables after oral appliance therapy (t-tests). |
{kind=link}
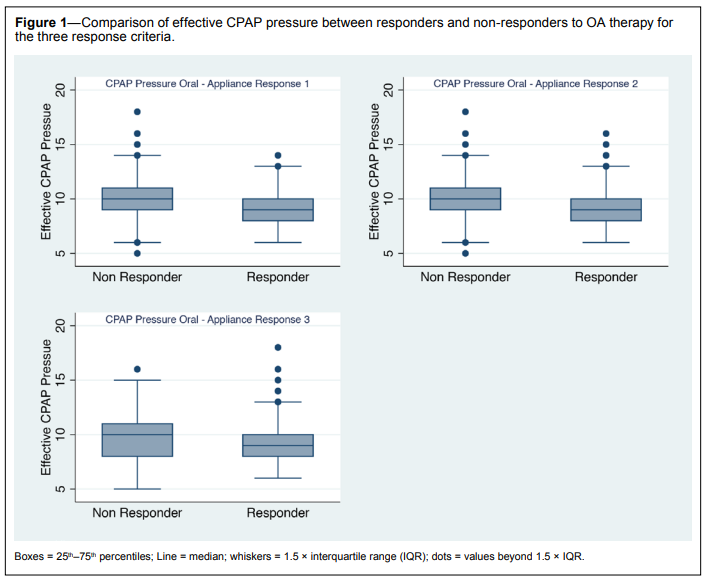
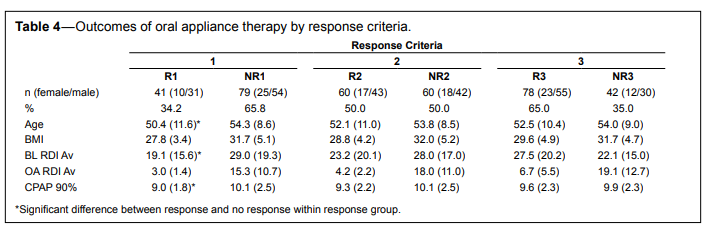
Complete response to OA therapy ranged from 34% to 65% of subjects, depending on response criteria (Figure 1). Only within response criterion 1 were there significant differences between responders and non-responders in age, baseline RDI and CPAP 90% pressure variables (Table 4). CPAP pressure was lower for responders versus non-responders by criteria 2 and 3 but was not statistically significant.
Figure 1Comparison of effective CPAP pressure between responders and non-responders to OA therapy for the three response criteria. |
{kind=link}
Table 4Outcomes of oral appliance therapy by response criteria. |
{kind=link}
Univariate logistic regression analysis by response criterion 1, using response as the dependent or outcome variable and CPAP pressure as the independent or predictor variable, was able to predict non-response based on CPAP pressure (AUC = 0.64, odds ratio = 1.27, 95% CI = 0.54–0.74, p < 0.02). Table 5 details the univariate regression models for the 3 response criteria.
Table 5Univariate logistic regression analyses for prediction of OA non-response with effective CPAP pressure. |
{kind=link}
A cut point, chosen to maximize sensitivity and specificity, of 9 cm of CPAP pressure correctly predicted 65.8% (sensitivity 76%, specificity 46%, positive/negative likelihood ratio 1.42/0.52) of response to OA therapy. A multivariate model that included BMI as well as 90% CPAP pressure correctly classified 74.1% of responders.
DISCUSSION
This is to date the largest study exploring the relationship between CPAP pressure and oral appliance outcome. In this study, CPAP pressure was statistically significantly predictive of oral appliance outcome only using the strictest definition of success (RDI < 5 and a reduction from baseline of at least 50%). This finding is in contrast to Sutherland,25 who found that CPAP pressure was predictive if criteria 2 and 3 were the definitions of response, but not if criterion 1 was the response definition. The differences in study populations and clinic processes may account for the differences. The baseline BMI of the subjects in the present study was 30.5 ± 5.0 kg/m2 , slightly larger than the subjects in Sutherland’s study (29.1 ± 5.8 kg/m2) 25 and significantly larger than those in the Tsuiki study (median 26 kg/m2).24
Fifty percent of the subjects in the present study were not tolerant of CPAP. This is in contrast to the previous studies. Those in the Tsuiki study were tolerant of CPAP for at least three months prior to fabricating the oral appliance.24 Those in the Sutherland study had a month adaptation to CPAP prior to the study.25 Possibly the previous experience of failure with CPAP influenced the outcome with the OA in the present study. The percentages of responders to OA therapy by criteria 1, 2, and 3 were 34.2%, 50.0%, and 65.0%. This response is similar to that found by Tsuiki (29%, 40%, and 63%) but less than response in the Sutherland study (53%, 69%, and 80%). Subjects in the present study were diagnosed and evaluated by level 3 or 4 sleep test. This protocol did not change over the study period. The previous studies used PSG for diagnosis and outcome evaluation. Although the sleep test methods differed, the response criteria were the same for all studies. Ours was a retrospective study of clinical patients who had chosen oral appliance therapy over CPAP, in addition to CPAP, or who were intolerant of CPAP. Patients used a variety of oral appliance designs over a longer clinical period than in the previous clinical studies Tsuiki found a significant relationship between CPAP pressure and all 3 response criteria in a smaller study of less overweight Japanese subjects. Tsuiki concluded that a CPAP pressure of 10.5 with a sensitivity/specificity of 90/56 was optimal for predicting response to oral appliance therapy.24 In our study, 9 cm was the optimal cut point, but our sensitivity/ specificity (76/46) was considerably weaker.
Differences in the CPAP pressures used could have lead to a variation in results. In our clinical environment many patients were on auto-CPAP and 90% pressures are determined by CPAP downloads. Both previous studies confirmed CPAP pressures with PSG. Sutherland25 used the 95th percentile rather than the 90th as is routinely used in our clinic. Our study had the additional variation introduced by a multiplicity of CPAP machines and oral appliances whereas in previous studies all patients used the same CPAP and oral appliance design.
The limitations of our study include the retrospective design and the variation introduced by the clinical situation. The patients were evaluated after a variety of acclimation and treatment times and having used a variety of oral appliances and CPAP machines. As the CPAP machines were primarily autotitrating and by a single manufacturer, it was not possible to do an analysis comparing the results by type of CPAP machine.
Despite the limitations of the study, the findings echo the previous studies conducted under more controlled conditions. CPAP pressure is a weak predictor of oral appliance outcome but when combined with BMI can be another clinical tool to help guide treatment decisions.
There are temporary appliances that can be used during a PSG to predict oral appliance outcomes.20,30 The predictive capabilities of these devices is better than CPAP pressure but the additional temporary appliance and PSG add complexity to the process.
Predicting outcomes with oral appliances continues to be a challenge. Many patients present for oral appliance therapy having had a trial of CPAP and clinicians can use information from CPAP trials. CPAP pressure is associated with but does not appear to be a reliable predictor of OA outcome.
REFERENCES
2. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008;31:1071–8.
3. Flemons WW. Clinical practice. Obstructive sleep apnea. New Engl J Med 2002;347:498–504.
4. George CF. Reduction in motor vehicle collisions following treatment of sleep apnoea with nasal CPAP. Thorax 2001;56:508–12.
5. Young T, Peppard PE, Taheri S. Excess weight and sleep-disordered breathing. J Appl Physiol 2005;99:1592–9.
6. Young T, Skatrud J, Peppard PE. Risk factors for obstructive sleep apnea in adults. JAMA 2004;291:2013–6.
7. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240–3.
8. Oksenberg A, Silverberg DS, Arons E, Radwan H. The sleep supine position has a major effect on optimal nasal continuous positive airway pressure : relationship with rapid eye movements and non-rapid eye movements sleep, body mass index, respiratory disturbance index, and age. Chest 1999;116:1000–6.
9. Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: the challenge to effective treatment. Proc Am Thorac Soc 2008;5:173–8.
10. Ferguson KA, Cartwright R, Rogers R, Schmidt-Nowara W. Oral appliances for snoring and obstructive sleep apnea: a review. Sleep 2006;29:244–62.
11. Ferguson KA, Ono T, Lowe AA, Keenan SP, Fleetham JA. A randomized crossover study of an oral appliance vs nasal-continuous positive airway pressure in the treatment of mild-moderate obstructive sleep apnea. Chest 1996;109:1269–75.
12. Lowe AA, Sjoholm TT, Ryan CF, Fleetham JA, Ferguson KA, Remmers JE. Treatment, airway and compliance effects of a titratable oral appliance. Sleep 2000;23 Suppl 4:S172–8.
13. Mehta A, Qian J, Petocz P, Darendeliler MA, Cistulli PA. A randomized, controlled study of a mandibular advancement splint for obstructive sleep apnea. Am J Respir Crit Care Med 2001;163:1457–61.
14. Gotsopoulos H, Chen C, Qian J, Cistulli PA. Oral appliance therapy improves symptoms in obstructive sleep apnea: a randomized, controlled trial. Am J Respir Crit Care Med 2002;166:743–8.
15. Hoekema A, Stegenga B, Bakker M, et al. Simulated driving in obstructive sleep apnoea-hypopnoea; effects of oral appliances and continuous positive airway pressure. Sleep Breath 2007;11:129–38.
16. Gotsopoulos H, Kelly JJ, Cistulli PA. Oral appliance therapy reduces blood pressure in obstructive sleep apnea: a randomized, controlled trial. Sleep 2004;27:934–41.
17. Naismith SL, Winter VR, Hickie IB, Cistulli PA. Effect of oral appliance therapy on neurobehavioral functioning in obstructive sleep apnea: a randomized controlled trial. J Clin Sleep Med 2005;1:374–80.
18. Hoekema A, Voors AA, Wijkstra PJ, et al. Effects of oral appliances and CPAP on the left ventricle and natriuretic peptides. Int J Cardiol 2008;128:232–9.
19. Hoekema A, Doff MH, de Bont LG, et al. Predictors of obstructive sleep apnea-hypopnea treatment outcome. J Dent Res 2007;86:1181–6.
20. Dort LC, Hadjuk E, Remmers JE. Mandibular advancement and obstructive sleep apnoea: a method for determining effective mandibular protrusion. Eur Respir J 2006;27:1003–9.
21. Tsai WH, Vazquez JC, Oshima T, et al. Remotely controlled mandibular positioner predicts efficacy of oral appliances in sleep apnea. Am J Respir Crit Care Med 2004;170:366–70.
22. Loredo JS, Berry C, Nelesen RA, Dimsdale JE. Prediction of continuous positive airway pressure in obstructive sleep apnea. Sleep Breath 2007;11:45–51.
23. Tsuiki S, Ito E, Isono S, et al. Oropharyngeal crowding and obesity as predictors of oral appliance treatment response to moderate obstructive sleep apnea. Chest 2013;144:558–63.
24. Tsuiki S, Kobayashi M, Namba K, et al. Optimal positive airway pressure predicts oral appliance response to sleep apnoea. Eur Respir J 2010;35:1098–105.
25. Sutherland K, Phillips CL, Davies A, et al. CPAP pressure for prediction of oral appliance treatment response in obstructive sleep apnea. J Clin Sleep Med 2014;10:943–9.
26. Eveloff SE, Rosenberg CL, Carlisle CC, Millman RP. Efficacy of a Herbst mandibular advancement device in obstructive sleep apnea. Am J Respir Crit Care Med 1994;149:905–9.
27. Henke KG, Frantz DE, Kuna ST. An oral elastic mandibular advancement device for obstructive sleep apnea. Am J Respir Crit Care Med 2000;161:420–5.
28. Dort L, Brant R. A randomized, controlled, crossover study of a noncustomized tongue retaining device for sleep disordered breathing. Sleep Breath 2008;12:369–73.
29. Pancer J, Al-Faifi S, Al-Faifi M, Hoffstein V. Evaluation of variable mandibular advancement appliance for treatment of snoring and sleep apnea. Chest 1999;116:1511–8.
30. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep 2013;36:1517–25.
ACKNOWLEDGMENTS
The authors thank Richard Hemsing for help with database development
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication August, 2015
Submitted in final revised form June, 2016
Accepted for publication August, 2016
Address correspondence to: Leslie Dort, DDS, 2716-7th Ave NW, Calgary, AB Canada T2N 1A7; Tel: (403) 686-4339; Fax: (403) 202-0266; Email: lcdort@gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Leslie Dort is Editor-inChief of the Journal of Dental Sleep Medicine. The authors have indicated no financial conflicts of interest.
PDF