Original Article 1, Issue 2.2
The Effects of an Oral Appliance in Obstructive Sleep Apnea Patients with Prehypertension
http://dx.doi.org/10.15331/jdsm.4630
Akshay Bhushan, MDS1 ; Arvind Tripathi, MDS, FACS, MNAMS, FICD1 ; Ashutosh Gupta, BDS1 ; Suryakant Tripathi, MD, FCCP, MNAMS2
1Department of Prosthodontics, Saraswati Dental College and Hospital, Lucknow, India; 2Department of Pulmonary Medicine, King George’s Medical University, Lucknow, India
ABSTRACT
Study Objectives:
The present study was aimed at estimating the effect of oral appliance treatment on the blood pressure of a cohort of obstructive sleep apnea (OSA) patients on a short-term (3 months) and long-term (1 year) basis and also to evaluate changes in the apnea-hypopnea index (AHI), snoring index (SI) and overall impact on the sleep apnea quality of life (SAQOL).
Methods:
37 patients who fulfilled the study criteria, underwent polysomnography before treatment with oral appliance, and then at 3 months and at 1 year after insertion of the oral appliance. Both systolic and diastolic blood pressure was recorded before treatment, at 3 months, and 1 year after insertion of oral appliance.
Results:
A decrease of 9.35% in systolic blood pressure (SBP) and 11.04% in diastolic blood pressure (DBP) of the patients was recorded after 3 months of continuous use of the oral appliance. Snoring index (SI) and AHI decreased by 80.31% and 83.93%, respectively, at the end of this period. A phenomenal increase in sleep apnea quality of life scores (183.9%) was observed in this time interval. The long-term efficacy of oral appliance use was evaluated at 1 year. There was a decrease of 12.16% in SBP and 14.01% in DBP and a decrease of 82.52% in AHI and 89.77% in SI scores. The level of improvement in SAQOL was 240% at the end of a year.
Conclusions:
There was a marked improvement in all symptoms observed, i.e., blood pressure, SI, and AHI indices and sleep apnea quality of life (after 3 months), which continued even on a long-term basis (at 1 year).
Keywords:
obstructive sleep apnea, mandibular advancement device, apnea-hypopnea index, snoring index, sleep apnea quality of life
Citation:
Bhushan A, Tripathi A, Gupta A, Tripathi S. The effects of an oral appliance in obstructive sleep apnea patients with prehypertension. Journal of Dental Sleep Medicine 2015;2(2):37–43.
Obstructive sleep apnea (OSA) syndrome is a serious condition that afflicts a substantial number of individuals. It is characterized by disruption of normal sleep architecture due to complete or partial obstruction of respiratory airflow. Airflow obstruction results in reduction of blood oxygen saturation also known as hypoxemia. It produces arousal in an attempt to reopen the airway. These recurring arousals disrupt the sleep architecture, leading to excessive daytime somnolence and poor quality of life.1 The worldwide OSA prevalence rates in adults ranges between 3.5% and 27%.2–3 In India, its prevalence ranges between 3% and 28% in men and 2.2% and 16% in women.4–5
It is well documented that OSA is associated with systemic hypertension, pulmonary hypertension, cardiac arrhythmia, ischemic heart disease, and stroke.6–11 Hypertension has been shown to occur in 28% to 57% of OSA patients, and there is a positive correlation between blood pressure and severity of apnea.12–15 Systemic blood pressure may increase by 20% immediately after an apneic episode and then rapidly fall to normal values after onset of respiration.16,17 Changes in blood pressure during the night may also influence morning blood pressure, which is usually higher in patients with OSA than normal subjects.18
During the last two decades there has been an increased interest in oral appliance as a treatment modality for OSA.19 The oral appliance is used during night; it protrudes the mandible and thereby opens the airway. The oral appliance is easy to use as it does not require electrical power, does not make any noise, and crossover studies have shown that patients prefer oral appliance therapy to CPAP, which leads to good compliance.20
The aim of this study was to estimate the effect of oral appliance treatment of OSA on blood pressure for short-term (3 months) and long-term (1 year) follow-up and to evaluate whether oral appliance treatment effected a decrease in apnea-hypopnea index (AHI) and snoring index (SI) and brought about an improvement in the sleep apnea quality of life (SAQOL).
METHODS
The present study was conducted in the Department of Prosthodontics, Saraswati Dental College & Hospital, Lucknow, in collaboration with Department of Pulmonary Medicine, King George’s Medical University, Lucknow. Prior approval of the institutional ethical committee (SDC-IHEC approval no. 018) had been obtained.
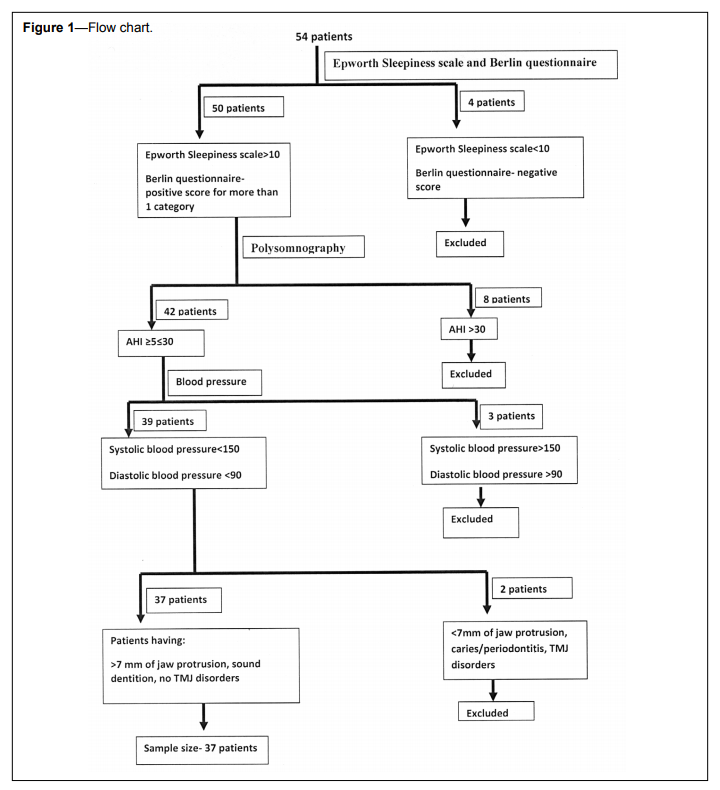
The inclusion criteria were:
- OSA verified by somnographic evaluation (defined as apnea-hypopnea index > 5 < 30 per hour) and ≥ 2 of the following symptoms: daytime sleepiness, snoring, witnessed apneas, and fragmented sleep.
- At least 7 mm of sustainable protrusive jaw movement from the position of maximum intercuspation.21
- More than 1 missing tooth per quadrant (excluding the third molar) that could minimize retention for the mandibular protruding device.
- Substantial evidence of TMJ disorders including pain, significant joint crepitation, restricted mouth opening, or sites of muscle tenderness in the masseter or temporalis region.22
- Severe caries and/or compromised periodontal status, which would not allow prolonged use of mandibular protruding device.
- Systolic blood pressure > 150 mm Hg or diastolic blood pressure > 90 mm Hg.
Figure 1Flow chart. |
{kind=link}
All patients were given custom-made mandibular advancement devices (MAD) as described by Napankangas et al.22 The range of mandibular advancement was set to 50% of maximum protrusive movement (mean 7 mm) since it was the maximum comfortable protrusion that was achieved with this mandibular advancement device.22
Blood pressure was measured between 09:00 and 11:00 and was measured before treatment, at 3 months, and at 1 year. All measurements (SBP and DBP) were done by the same operator using sphygmomanometer. During the clinical blood pressure measurement, the patients were reclined in a supine position with the arm at heart level. Three readings were taken at each sitting and averaged to obtain a single value for SBP and DBP, respectively.
Polysomnography
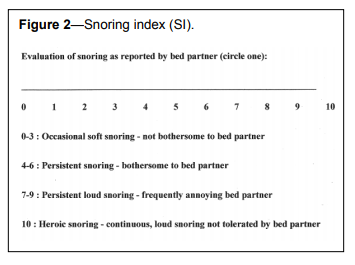
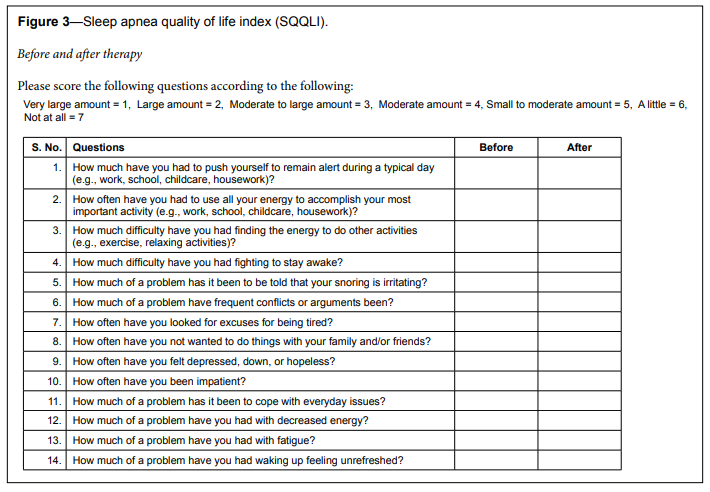
Overnight polysomnography (S-7000, Cogent technologies, EMBLA System Inc) included electroencephalograms (EEG: C3-A2, C4-A1, O2-A1, O3-A2), bilateral electro-oculogram (ROC, LOC), chin and leg electromyogram (EMG), nasal airflow, thoracic and abdominal movements, electrocardiogram (ECG), and body position recorders. AHI was calculated with the help of Somnologica studio software. The apnea episodes were defined as complete cessation of airflow for ≥ 10 s; hypopnea was defined as ≥ 50% reduction in oronasal airflow accompanied by a reduction ≥ 4% oxygen saturation calculated by pulse oximetry.23 AHI was determined by the frequency of these events per hour during sleep time based on the results of the overnight polysomnography. Recorded polysomnographic data were cross-checked manually for apneas and hypopnea events.For grading of snoring intensity, the bed partner snoring evaluation index tool24,25 was used (Figure 2). Sleep apnea quality of life index (SAQLI)26 was used to assess the SAQOL of the patients (Figure 3).
Figure 2Snoring index (SI). |
{kind=link}
Figure 3Sleep apnea quality of life index (SQQLI). |
{kind=link}
To determine the course of analysis, all data obtained were subjected to test of normality using Kolmogorov-Smirnov test. The analytical plan was dependent on the symmetry of data obtained. It was planned that if all the parameters recorded had a normal distribution, a parametric plan would be followed; otherwise a nonparametric plan was the choice. Data were analyzed using Statistical Package for Social Sciences, version 15.0. Wilcoxon signed rank test was used to evaluate before-after changes. A P value < 0.05 indicated statistically significant difference.
RESULTS
On evaluating the distribution for normality (before treatment), only blood pressure, AHI, SI were found to be normal and hence a nonparametric analysis plan was adopted (Table 1).Table 1Test for normality (Kolmogorov-Smirnov Test). |
{kind=link}
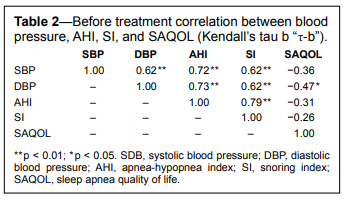
Table 2 shows the correlation between blood pressure, AHI, SI and SAQOL. This correlation was explored using the Kendall’s tau-b (nonparametric variant of Pearson correlation coefficient). SBP had a moderate positive correlation with DBP (τ = 0.62) and SI (τ = 0.62) whereas the correlation with SBP and AHI was positive and strong (τ = 0.72). However, the correlation between SBP and SAQOL was inverse and mild (τ = −0.36). DBP had moderate positive correlation with SBP (τ = 0.62) and snoring index (τ = 0.62) and a strong correlation with AHI (τ = 0.73). The correlation between DBP and SAQOL was inverse and mild (τ = −0.47).
AHI had a strong positive correlation with SBP (τ = 0.72), DBP (τ = 0.73), and snoring index (τ = 0.79), and a mild inverse correlation (τ = −0.31) with SAQOL scores. Snoring index had a moderate positive correlation with SBP and DBP (τ = 0.62) and a strong correlation with AHI (τ = 0.79). The correlation between snoring index and SAQOL was inverse and weak in nature (τ = −0.26).SAQOL had mild inverse correlation with SBP, DBP, and AHI (τ = −0.3 to −0.5) and a weak inverse correlation with snoring index (τ = −0.26) (Table 2).
Table 2Before treatment correlation between blood pressure, AHI, SI, and SAQOL (Kendall’s tau b “τ-b”). |
{kind=link}
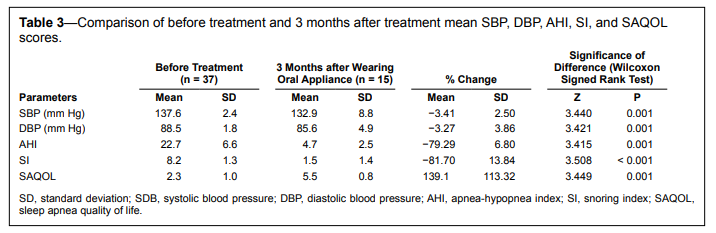
A significant reduction in mean SBP, DBP, AHI, and SI was observed after 3 months of wearing oral appliance (P ≤ 0.001), whereas a significant increase in sleep apnea quality of life score was observed (P = 0.001). Among all variables, maximum proportional change was observed in SAQOL scores where an increase of 139.1% ± 113.32% (mean ± standard deviation [SD]) (from 2.3 preoperative to 5.5 after 3 months) was observed, whereas minimum change was observed in DBP (mean ± SD decrease of 3.27% ± 3.86%; Table 3).
Table 3Comparison of before treatment and 3 months after treatment mean SBP, DBP, AHI, SI, and SAQOL scores. |
{kind=link}
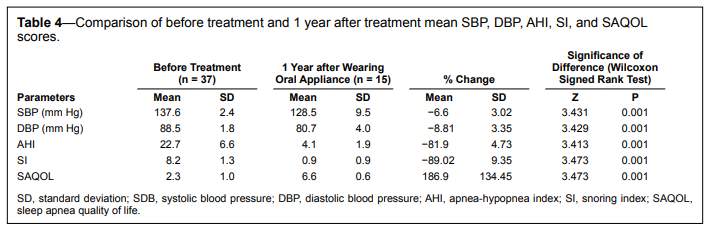
A significant reduction in mean SBP, DBP, AHI, and SI was observed at 1 year treatment interval as compared to pretreatment values (P = 0.001), whereas a significant increase in SAQOL scores was observed (P = 0.001) after 1 year of wearing oral appliance. Among all variables, maximum proportional change was observed in SAQOL scores, where an increase of 186.9% ± 134.45% (from 2.3 preoperative to 6.6 after 1 year) was observed; minimum change was observed in SBP (Table 4).
Table 4Comparison of before treatment and 1 year after treatment mean SBP, DBP, AHI, SI, and SAQOL scores. |
{kind=link}
DISCUSSION
The present study was aimed at estimating the effect of oral appliance treatment on the blood pressure on a cohort of OSA patients on a short-term (3 months) and long-term (1 year) basis and also to evaluate changes in the AHI index, snoring index, and the overall impact on the sleep apnea quality of life. For this, 37 prehypertensive dentulous patients falling into the category of mild-to-moderate OSA with sound dentition (caries/periodontitis free) and without any sign or symptoms of temporomandibular disorder were selected. Prehypertension is a systolic pressure from 120 to 139 mm Hg or a diastolic pressure from 80 to 89 mm Hg.27 Prehypertension can be corrected with lifestyle modification and does not require hypertensive drug therapy; to eliminate the bias of hypertensive drug, only those patients that were not taking any hypertensive medication and falling into the prehypertension category were selected.27 All these patients were given custom-made mandibular advancement devices.22 Oral appliances are successful in individuals with mild-to-moderate OSA but have been proven less effective for severe cases.28 In one study comparing CPAP to dental appliance in mild-to-moderate OSA, dental appliances decreased AHI from 21 to 14, compared to a decreased AHI of 5 in patients using CPAP.29 Oral appliances serve to advance the mandible within a range of physiological limits along the path of condylar guidance and bring about an increase in the volume of the hypopharynx. Any temporomandibular disorder (including pain, significant joint crepitation, restricted mouth opening, or sites of muscle tenderness in the masseter or temporalis region) would prevent smooth gliding of the mandible; hence patients having TMDs and AHI > 30 were excluded.22
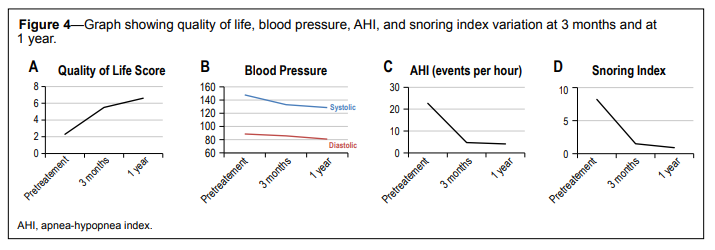
It was interesting to note that the profound improvement was observed in SI, AHI, and blood pressure after 3 months of oral appliance use, which became less marked in profile in the next 9 months. However SAQOL scores showed a steady upward trend (Figure 4).
Figure 4Graph showing quality of life, blood pressure, AHI, and snoring index variation at 3 months and at 1 year. |
{kind=link}
Otsuka et al. showed a significant reduction in SBP (from 118.4 to 113.7) and DBP (from 71.6 to 67.2) following the use of oral appliance.30 The study suggested that successful OSA treatment with an oral appliance may also be beneficial to lower blood pressure in OSA patients, as previously suggested for nasal continuous positive airway pressure therapy.
Becker et al. showed that active CPAP treatment resulted in a pronounced reduction in daytime and nighttime blood pressure (blood pressure reduction of 8.1 and 11.4 mm Hg for SBP and DBP), a result comparable to those of the present study.31
There are conflicting data in the literature on the impact of CPAP on blood pressure, with some studies reporting limited or no effect while others have found benefit.32–38 This may be because compliance with oral appliance is much higher than compliance with CPAP.
Zang et al. showed that after a 12-week treatment, an oral appliance group showed significant reduction in nocturnal mean SBP and DBP, and 24-h and diurnal SBP ([121.3 ± 7.0] vs [125.3 ± 9.3], [76.1 ± 6.1] vs [78.8 ± 6.8], [127.2 ± 7.5] vs [129.4 ± 8.8], and [131.5 ± 6.9] vs [133.6 ± 8.1], respectively, all P < 0.01).3
A systematic review incorporating seven studies on effect of oral appliance on blood pressure in patients with OSA by Iftikhar et al.39 showed that the pooled mean change in the SBP, DBP, and the MAP (mean arterial blood pressure) were −2.7 mm Hg, −2.7 mm Hg, and −2.40 mm Hg, respectively, showing that effective oral appliance therapy can bring about reduction in SBP, DBP, and MAP
Sleep apnea quality of life is an objective measurement of a combined state of well-being in an individual and is dependent on a multitude of factors. There is evidence that altered health is often accompanied by psychological distress that hampers the quality of life.40 A minor elevation in health status might influence the quality of life tremendously. The findings in the present study also support this assumption, as we observed almost 240% rise in sleep apnea quality of life of patients with a change of 12.16% and 14.01% in SBP and DBP and a change of 82.52% and 89.77% in AHI and SI scores.
Limitations of this study include the absence of any controls, as it was unethical to leave hypertensive patients untreated for 1 year. Another limitation was the effect of lifestyle factors, intake of caffeine and alcohol, and presence of obesity, which were not part of the study. All the patients were regularly recalled, and most of them did not report any discomfort with mandibular advancement device. However, in a few patients, altered maxillomandibular relationships (due to mandibular advancement) could cause impingement of the dental prosthesis in newer areas. In this event, such areas were identified and the MAD was suitably modified to prevent further impingement.
CONCLUSION
The result of the present study suggests that oral appliance can reduce blood pressure and can bring a radical change in blood pressure, apnea-hypopnea index, snoring index, and sleep apnea quality of life within a short period (3 months) and has the ability to sustain this trend in the long run (1 year).REFERENCES
2. Young TM, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. New Engl J Med 1993;328:1230–5.
3. Garcia-Rio F, Racionero MA, Pino JM, et al. Sleep apnea and hypertension. Chest 2000;117:1417–25.
4. Lam JC, Sharma SK, Lam B. Obstructive sleep apnoea: definitions, epidemiology & natural history. Indian J Med Res 2010;131:165–70.
5. Reddy EV, Kadhiravan T, Mishra HK, et al. Prevalence and risk factors of OSA in Middle aged urban Indians: a community based study. Sleep Med 2009;10:913–8
6. Millmann RP, Redline S, Carslisle C, et al. Daytime hypertension in obstructive sleep apnea. Prevalence and contributing factors. Chest 1991;99:861–6.
7. Weitzenblum E, Kriege J, Apprill M, et al. Daytime pulmonary hypertension in patients with obstructive sleep apnea syndrome. Am Rev Respir Dis 1988;138:345–9.
8. Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia and conductance disturbances during sleep in 400 patients with sleep apnea syndrome. Am J Cardiol 1983;52:490–4.
9. Gonzalez-Rothi R, Foresman GE, Block AJ. Do patients with sleep apnea die in their sleep? Chest 1988;94:531–8.
10. Partinen M, Guilleminault C. Daytime sleepiness and vascular morbidity at seven-year follow-up in obstructive sleep apnea patients. Chest 1990;97:27–32.
11. Palomaki H. Snoring and the risk of ischemic brain infarction. Stroke 1991;22:1021–5.
12. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med 2000;342:1378–84.
13. Lavie P, Herer P, Hoffstein V. Obstructive sleep apnea syndrome as a risk factor for hypertension: population study. BMJ 2000;320:479–82.
14. Grote L, Ploch T, Hietmann J, Knaack L, Penzel T, Peter JH. Sleeprelated breathing disorder is an independent risk factor for systemic hypertension. Am J Respir Crit Care Med 1999;160:1875–82.
15. Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertension in large community-based study. JAMA 2000;283:1829–36.
16. Stoohs R, Guilleminault C. Cardiovascular changes associated with obstructive sleep apnea syndrome. J Appl Physiol 1992;72:583–9.
17. Coccagna G, Mantovani M, Brignani F, Parchi C, Lugaresi E. Continuous recording of the pulmonary and systemic arterial pressure during sleep in syndromes of hypersomnia with periodic breathing. Bull Physiopathol Respir 1972;8:1159–72
18. Calhoun AD, Harding MS. Sleep and hypertension. Chest 2010;138:434– 43.
19. Andrén A, Hedberg P, Walker-Engström ML, Wahlén P, Tegelberg A. Effects of treatment with oral appliance on 24-h blood pressure in patients with obstructive sleep apnea and hypertension: a randomized clinical trial. Sleep Breath 2013;17:705–12.
20. Chan AS, Cistulli PA. Oral appliance treatment of obstructive sleep apnea: an update. Curr Opin Pulm Med 2009;15:591–6.
21. Vanderveken OM, Van de Heyning PH, Braem MJ. effects of vertical opening on pharyngeal dimensions in patients with obstructive sleep apnea. Sleep Med 2012;13:314–6.
22. Napankangas R, Sipila K, Raustia A. Effect of mandibular advancement device therapy on the signs and symptoms of temporomandibular disorders. J Oral Maxillofac Res 2012;3:e5.
23. Garg R, Singh A, Prasad R, Saheer S, Jabeed P, Verma R. A comparative study on the clinical and polysomnographic pattern of obstructive sleep apnea among obese and non-obese subjects. Ann Thorac Med 2012;7:26– 30.
24. Hofmann T, Schwantzer G, Reckenzaun E, Koch H, Wolf G. Radiofrequency tissue volume reduction of the soft palate and UPPP in the treatment of snoring. Eur Arch Otorhinolaryngol 2006;263:164–70.
25. Tripathi A, Gupta A, Tripathi S, Dubey A. A novel use of complete denture prosthesis as mandibular advancement device in the treatment of obstructive sleep apnea in edentulous subjects. J Dent Sleep Med 2014;1:115–9.
26. Sharples L, Glover M, Clutterbuck-James A, et al. Clinical effectiveness and cost-effectiveness results from the randomised controlled Trial of Oral Mandibular Advancement Devices for Obstructive sleep apnoeahypopnea (TOMADO) and long-term economic analysis of oral devices and continuous positive airway pressure. Southampton (UK): NIHR Journals Library; 2014 Oct. (Health Technology Assessment. No. 18.67.) Appendix 3, Sleep Apnoea Quality of Life Index.
27. Chobanian AV, Bakris GL, Black HR, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 2003;289:2560–72.
28. Machado M, Juliano L, Taga M, et al. Titratable mandibular repositioner appliances for obstructive sleep apnea syndrome: are they an option? Sleep Breath 2007;11:225–31.
29. Barnes M, McEvoy R, Banks S, et al. Efficacy of positive airway and oral appliance in mild to moderate obstructive sleep apnea. Am J Resp Crit Care Med 2004;170:656–64.
30. Otsuka R, Ribeiro de Almeida F, Lowe AA, Linden W, Ryan F. The effect of oral appliance therapy on blood pressure in patients with obstructive sleep apnea. Sleep Breath 2006;10:29–36.
31. Becker HF, Jerrentrup A, Ploch T, et al. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive with obstructive sleep apnea. Circulation 2003;107:68–73.
32. Faccenda JF, Mackay TW, Boon NA, Douglas NJ. Randomized placebocontrolled trial of continuous positive airway pressure on blood pressure in the sleep apnea-hypopnea syndrome. Am J Respir Crit Care Med 2001;163:344–8.
33. Pepperell JC, Ramdassingh-Dow S, Crosthwaite N et al. Ambulatory blood pressure after therapeutic and subtherapeutic nasal continuous positive airway pressure for obstructive sleep apnoea: a randomised parallel trial. Lancet 2002;359:204–10.
34. Becker HF, Jerrentrup A, Ploch T, et al. Effect of nasal continuous positive airway pressure treatment on blood pressure in patients with obstructive sleep apnea. Circulation 2003;107:68–73.
35. Engleman HM, Gough K, Martin SE, Kingshott RN, Padfield PL, Douglas NJ. Ambulatory blood pressure on and off continuous positive airway pressure therapy for the sleep apnea/hypopnea syndrome: effects in “non-dippers.” Sleep 1996;19:378–81.
36. Dimsdale JE, Loredo JS, Profant J. Effect of continuous positive airway pressure on blood pressure: a placebo trial. Hypertension 2000;35:144–7.
37. Barbe F, Mayoralas LR, Duran J, et al. Treatment with continuous positive airway pressure is not effective in patients with sleep apnea but no daytime sleepiness: A randomized, controlled trial. Ann Intern Med 2001;134:1015–23.
38. Zhang LQ, Zheng X, Wang JL, Wang YZ, Ren B, He B. Effects of oral appliance treatment upon blood pressure in mild to moderate obstructive sleep apnea-hypopnea syndrome. Zhonghua Yi Xue Za Zhi 2009;89:1807–10.
39. Iftikhar IH, Hays ER, Iverson MA, Magalang UJ, Maas AK. Effect of oral appliances on blood pressure in obstructive sleep apnea: a systematic review and meta-analysis. J Clin Sleep Med 2013;9:165–74.
40. Tajvar M, Arab M, Montazeri A. Determinants of health-related quality of life in elderly in Tehran, Iran. BMC Public Health 2008;8:323.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication December, 2014
Submitted in final revised form February, 2015
Accepted for publication February, 2015
Address correspondence to: Dr. Arvind Tripathi, MD 10, Sector C, Aliganj, Lucknow 226 024, Uttar Pradesh, India; Email: atrip2006@gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest. The work was performed at the Department of Prosthodontics, Saraswati Dental College & Hospital, Lucknow and Department of Pulmonary Medicine, King George’s Medical University, Lucknow, India.
PDF