Original Article 1, Issue 1.3
A Novel Use of Complete Denture Prosthesis as Mandibular Advancement Device in the Treatment of Obstructive Sleep Apnea in Edentulous Subjects
http://dx.doi.org/10.15331/jdsm.4134
Arvind Tripathi, MDS, FACS1 ; Ashutosh Gupta, BDS1 ; Suryakant Tripathi, MD, FCCP2 ; Abhishek Dubey, MSc3
1Saraswati Dental College and Hospital, Lucknow, India; Saraswati Dental College and Hospital, Lucknow; 2 Department of Pulmonary Medicine, King George’s Medical University, Lucknow, India; 3 PhD Scholar at King George’s Medical University, Lucknow, India
ABSTRACT
Study Objective:
Mandibular advancement devices have been used to efficiently treat mild to moderate obstructive sleep apnea by effecting a forward positioning of the tongue- mandible complex and a resultant increase in oropharyngeal volume. These devices are essentially tooth anchored and hence, work well in dentate patients. However, it is difficult to anchor such devices in an edentate mouth. This clinical study presents a case series on use of complete dentures modified to function as mandibular advancement device.
Methods:
Ten edentulous OSA patients (8 male and 2 female, aged 61 ± 4 years; BMI 22 ± 5; AHI 15-30) who volunteered and provided written informed consent were included in the study. All of them were provided with complete dentures, and after 1 month of comfortable wear and attaining optimum function, the prosthesis was modified to serve alternatively as a mandibular advancement device. Use of complete dentures as MAD was recorded separately. Five variables were assessed preoperatively and after 6 months of wearing the modified mandibular advancement device. The variables were: sleep efficiency, apnea-hypopnea index, oxygen desaturation events/h, mean O2 saturation, and snoring index. Overnight polysomnography was done to evaluate the sleep variables preoperatively and after 6 months of wearing the modified mandibular advancement device.
Results:
A significant decrease in apnea-hypopnea index (AHI) from 22.5 preoperatively to 4.8 postoperatively (p = 0.005) and snoring index from 7.9 preoperatively to 2.1 postoperatively (p = 0.005) was observed after 6 months of use of the modified oral appliance. Sleep efficiency increased from 62.55% preoperatively to 73.20% postoperatively (p = 0.005).
Conclusions:
The results indicate that within the limits of the present study, this specific MAD can be effective in reducing sleep apnea by lowering the AHI, reducing snoring and oxygen desaturation events/h and increasing sleep efficiency.
Keywords:
mandibular advancement device, obstructive sleep apnea, complete edentulism
Citation:
Tripathi A, Gupta A, Tripathi S, Dubey A. A novel use of complete denture prosthesis as mandibular advancement device in the treatment of obstructive sleep apnea in edentulous subjects. Journal of Dental Sleep Medicine 2014;1(3):115–119.
Obstructive sleep apnea (OSA) syndrome is a serious medical condition that affects substantial number of individuals. The worldwide OSA prevalence rates in adults ranges between 3.5% to 27%.1,2 In India, its prevalence ranges between 3% and 28% in men and 2.2% and 16% in women.3-5 It is characterized by a disruption of normal sleep architecture due to partial or complete obstruction of the respiratory airflow. Airflow obstruction leads to a reduction of blood oxygen saturation, also known as hypoxemia. This produces an arousal in an attempt to reopen the airway. Recurrent arousals disrupt the sleep architecture, diminish the quality of sleep, and cause excessive daytime somnolence. These features have a deleterious effect on the quality of life and state of health of affected individuals.6
Studies suggest that edentulism worsens sleep apnea.7-9 Loss of vertical dimension of occlusion causes reduction of the lower facial height and rotation of the mandible. Sleeping without dentures may be associated with a significant increase in the AHI.7 The lack of a vertical stop facilitates an overclosure of the maxillomandibular system and an upper airway collapse. Even in a patient using complete dentures, the vertical dimension of occlusion worsens continuously because of bone resorption.2
During the last two decades, there has been increased interest in oral appliance (OA) as a treatment modality for OSA. The OA is used during night; it protrudes the mandible and thereby opens the airway. The oral appliance is easy to use as it does not require electrical power and does not make any noise; crossover studies have shown that patients prefer OA therapy to CPAP, which leads to good compliance.
Oral appliances can either be prefabricated or custom made. Custom-made mandibular advancement devices (MADs) are fabricated on dental casts of the patient. All MADs have been developed for dentate patients in whom the remaining dentition provides anchorage and stability to the device. Only tongue retaining devices (TRD) have been recommended for edentate patients.10-12 Earlier clinical studies on the use of dentures for the treatment of OSA13-15 have not reported data on mandibular advancement. This clinical study presents a case series on use of complete dentures modified to function as MAD.
METHODS
The present study was conducted in the Department of Prosthodontics, Saraswati Dental College & Hospital, Lucknow, in collaboration with Department of Pulmonary Medicine, King George’s Medical University, Lucknow. Prior approval of the Institutional ethical committee had been obtained.
Ten edentulous OSA patients (8 male, 2 female, age 61 ± 4 years; BMI 22 ± 5; AHI 15-30), who volunteered and provided written informed consent were included in the study. A provisional selection of patients was based on subjective evaluation of symptoms, according to the Epworth Sleepiness Scale and the Berlin Questionnaire. Such patients were subjected to overnight polysomnography to confirm their actual status before being included as study subjects. Five variables were assessed preoperatively and after 6 months of wearing the modified MAD. These variables were: sleep efficiency, AHI, oxygen desaturation events/h, mean O2 saturation, and snoring index.
For recording sleep efficiency, AHI, oxygen desaturation events/h, limb movement and mean O2 saturation, overnight polysomnography was performed twice (preoperatively and after 6 months of wearing the appliance).
Overnight polysomnography sleep study (S-7000, Cogent technologies, EMBLA System Inc) included electroencephalograms (EEG); (C3-A2, C4-A1, O2-A1, O3-A2), bilateral electrooculogram (ROC, LOC), chin and leg electromyogram (EMG), nasal airflow, thoracic and abdominal movements, electrocardiogram (ECG), O2 saturation measurement by finger pulse oximeter, and body position recorders. Apnea-hypopnea index (AHI) was calculated with the help of Somnologica Studio software. The apnea episodes were defined as complete cessation of airflow ≥ 10 s, and hypopnea was defined as ≥ 50% reduction in oronasal airflow accompanied by a reduction of ≥ 4% oxygen saturation calculated by pulse oximetry. AHI was determined by the frequency of these events per hour during sleep time based on the results of the overnight polysomnography. Recorded polysomnographic data were cross checked manually for scoring of sleep stages, apneas, and hypopnea events.
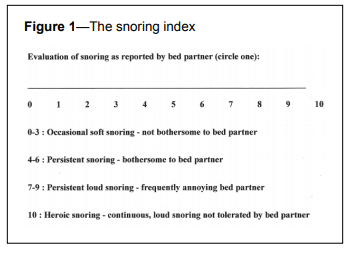
For grading of snoring intensity, the bed partner snoring evaluation index tool was used (Figure 1). As the sample size was small a nonparametric assessment plan was adopted. Data were analyzed using SPSS Version 15.0. Wilcoxon signed rank test was used to evaluate before-after changes. A p value < 0.05 indicated statistically significant difference.
Figure 1The snoring index |
{kind=link}
Complete Denture Prosthesis Modified To Function as a Mandibular Advancement Device
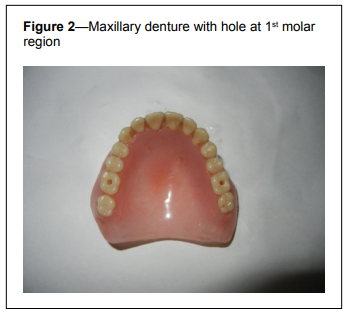
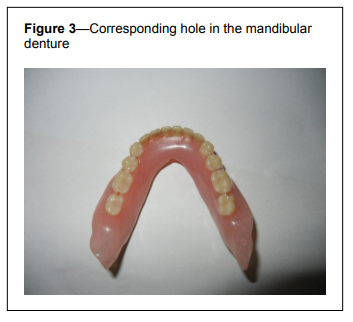
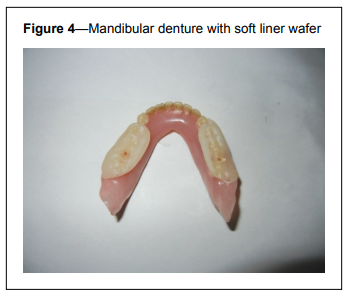
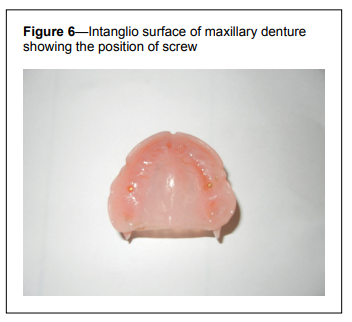
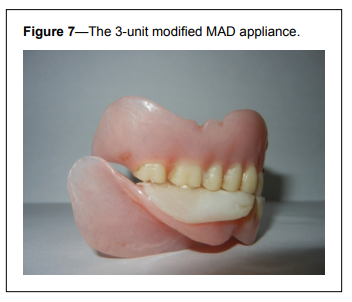
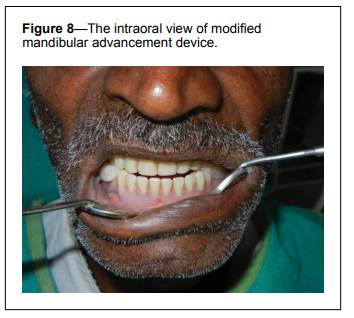
Maxillary and mandibular complete dentures were fabricated by the conventional standard procedure. With the maxillary denture in the patient’s mouth, facebow records were taken and transferred onto the Hanau “wide vue” articulator. A 3-mm thick wax interocclusal record was made and maximum protrusive jaw movement was done, as dictated by the condylar guidance path. The mandibular denture was mounted on the articulator using the wax record. The wax record was removed and the centric lock of the articulator was fixed at 70% of maximum protrusion.16 Next, the heat cure soft liner (Permasoft) was added on the occlusal surface from the first premolar up to the second molar. The articulator was closed and the soft liner was allowed to set. The soft liner wafer was then cured, and thereafter the entire assembly (the maxillary and mandibular dentures and the soft liner wafer) was removed from the articulator. A hole was drilled at the first molar region on the intaglio surface of maxillary denture bilaterally, passing through the soft liner wafer up to the occlusal surface of mandibular denture, such that the two could be engaged securely. The soft liner wafer was fixed to the maxillary and mandibular denture using brass screws passing through the hole. This was done so that dentures could provide the function of mastication by removing the wafer during the daytime and then function as a mandibular advancement prosthesis by placing the wafer and tightening it with screws during sleep at night. The wafer engaged the posterior occlusion and created an interarch anterior space, which facilitated unobstructed inspiration even during sleep. The 3-piece modified mandibular advancement device (maxillary and mandibular dentures with soft liner wafer in between), was inserted and adjusted intraorally. The patient was provided with a brass mini-screwdriver and was instructed on how to screw the denture and soft liner wafer during night and to unscrew it during daytime (Figures 2-8).Figure 2Maxillary denture with hole at 1st molar region |
{kind=link}
Figure 3Corresponding hole in the mandibular denture |
{kind=link}
Figure 4Mandibular denture with soft liner wafer |
{kind=link}
Figure 5The screw used to immobilize the denture and the soft liner wafer during night. |
{kind=link}
Figure 6Intanglio surface of maxillary denture showing the position of screw |
{kind=link}
Figure 7The 3-unit modified MAD appliance. |
{kind=link}
Figure 8The intraoral view of modified mandibular advancement device |
{kind=link}
RESULTS
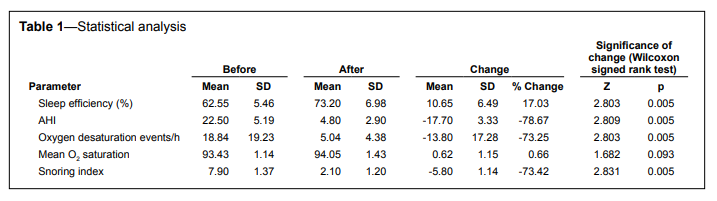
A significant decrease in AHI from 22.5 preoperatively to 4.8 postoperatively (78.67%), snoring index (from 7.9 preoperatively to 2.1 postoperatively [73.42%]) and oxygen desaturation events/h (from 18.84 preoperatively to 5.04 postoperatively) was observed after 6 months of wearing the modified oral appliance. Sleep efficiency increased from 62.55% preoperatively to 73.20% postoperatively. However, there was no statistically significant improvement in mean O2 saturation event (p value > 0.05; Table 1). For a mean change of 10.65 units with a pooled standard deviation of 6.49 units, the power of test was 100%.Table 1Statistical analysis |
{kind=link}
DISCUSSION
The present study found the use of complete dentures with modifications to be an effective mandibular advancement device for the treatment of obstructive sleep apnea in a sample of edentulous patients. The MAD was retained by the edentulous arches and stabilized by screwing on the interocclusal wafer with the maxillary and the mandibular dentures, thus rendering the three as one composite unit. Placement of the wafer between the dentures increased the interarch distance (vertically) enough to make the MAD appliance self-retentive even at rest. Since the MAD was a mere modified version of dentures already in use with no discomfort, no fresh complaint of soreness or ulceration was reported. The MAD was prepared at 70% of the maximum mandibular protrusion recorded, to avoid any possible anterior impingement of the glenoid fossae by the condyles as done by Keyf et al.16 Since the appliance was an altered form of a well-adjusted dental prosthesis, the patients did not report any discomfort. However, in certain cases, altered maxillomandibular relationship (due to mandibular advancement) may lead to impingement of dental prosthesis in newer areas and cause fresh denture soreness. In this event, such spots must be identified and the denture suitably modified to prevent any impingement. Further, since the denture prosthesis is being worn by the patient both during day and night, intaglio surface hygiene is of critical value and the patient must be suitably counselled on denture hygiene procedures. Increased vertical separation of the maxilla and the mandible when the dentures are used as MAD may cause initial discomfort, which is easily overcome by the patient in a couple of days.
The reason for setting the age limit of 61 ± 4 years for the study population was the higher chance of central sleep apnea in patients over this age, which could have otherwise provided false results. Gender distribution in the study was 80% men and 20% women. OSA is 3 to 4 times more prevalent in men than women, which may be related to differences in sex hormones and preferential fat distribution in women in the subcutaneous tissue of hips and thighs, with less deposition in the neck, in contrast to men.17,18
The efficacy of MAD in the treatment of edentulous patients with OSA has been reported in previous studies. In a study by Arisaka et al. comprising 34 OSA patients (AHI ≥ 5), the mean AHI in patients sleeping with dentures was lower than that of those without dentures (13.3 ± 10.0 versus 17.7 ± 14.6, p = 0.022).13 The result showed that 70% of the individuals showed marked improvement in AHI after wearing dentures. However, this study did not show the effect of denture advancement on sleep variables.
Erovigni et al. showed by cephalometric evaluation that wearing denture induces modifications in the position of the tongue, of the jaw, and of the pharyngeal airway space that can favor the reduction of apnea episodes.19
Recently, a few studies have shown that oral appliances could be used in partially and totally edentulous patients with OSA.20 Giannasi et al. applied an adjustable MAD on a maxillary edentulous patient with a dentate mandible.21 They reported a sharp decrease in AHI from 18.0 to 2.2/h. Nayar and Knox22 reported some advantages of an individually fabricated MAD on a totally edentulous patient with OSAS. They reported improvement of patient compliance based on subjective data (such as patient history) without polysomnography. Kurtulmus and Cotert fabricated a combination of TRD and MAD for a totally edentulous patient.23
CONCLUSIONS
The results indicate that within the limits of the present study, this specific MAD is effective in reducing sleep apnea by lowering the AHI and reducing snoring and oxygen desaturation events/h in a significant way along with improvement in sleep efficiency. The MAD has been well tolerated by all patients.REFERENCES
2. Garcia-Rio F, Racionero MA, Pino JM, et al. Sleep apnea and hypertension. Chest 2000;117:1417-25.
3. Sharma SK, Ahluwalia G. Epidemiology of adult obstructive sleep apnoea syndrome in India. Indian J Med Res 2010;131:171-5.
4. Lam JC, Sharma SK, Lam B. Obstructive sleep apnoea: definitions, epidemiology & natural history. Indian J Med Res 2010;131:165-5.
5. Reddy EV, Kadhiravan T, Mishra HK, et al. Prevalence and risk factors of OSA in middle-aged urban Indians: a community based study. Sleep Med 2009;10:913-8.
6. Young T, Palta M, Dempsey J, et al. Burden of sleep apnea: rationale, design, and major findings of the Wisconsin Sleep Cohort Study. WMJ 2009;108:246-9.
7. Bucca C, Cicolin A, Brussino L, et al. Tooth loss and obstructive sleep apnea. Respir Res 2006;7:8.
8. Ancoli-Israel S, Gehrman P, Kripke DF, et al. Long term follow up of sleep disordered breathing in older adults. Sleep Med 2001;2:511-6.
9. Ancoli-Israel S, Kripke DF, Klauber MR, et al. Sleep disordered breathing in community dwelling elderly. Sleep 1991;14:486-95.
10. Cistulli PA, Gotsopoulos H, Marklund M, Lowe AA. Treatment of snoring and obstructive sleep apnea with mandibular repositioning appliances. Sleep Med Rev 2004;8:443-57.
11. Chan AS, Cistulli PA. Oral appliance treatment of obstructive sleep apnea: an update. Curr Opin Pulm Med 2009;15:591-6.
12. Vanderveken OM, Devolder A, Marklund M, et al. Comparison of a custom-made and a thermoplastic oral appliance for the treatment of mild sleep apnea. Am J Respir Crit Care Med 2008;178:197-202.
13. Arisaka H, Sakuraba S, Tamaki K, Watanabe T, Takeda J, Yoshida K. Effects of wearing complete dentures during sleep on the apneahypopnea index. Int J Prosthodont 2009;22:173-7.
14. Meyer JB, Knudson RC. Fabrication of prosthesis to prevent sleep apnea in edentulous patients. J Prosthet Dent 1990;63:448-51.
15. Almeida FR, Furuyama RJ, Chaccur DC, et al. Complete denture wear during sleep in elderly sleep apnea patients: a preliminary study. Sleep Breath 2012;16:855-63.
16. Keyf F, Ciftci B, Guven FS. Management of obstructive sleep apnea in an edentulous lower jaw patient with a mandibular advancement device. Case Reports in Dentistry 2014;2014:436904.
17. Kapsimalis F, Kryger MH. Gender and obstructive sleep apnea syndrome, part 2: mechanism. Sleep 2002; 25:412-9.
18. Jamieson A, Guilleminault C, Partinen M, Quera-Salva MA. Obstructive sleep apneic patients have craniomandibular abnormalities. Sleep 1986;9:469-77.
19. Erovigni F, Graziano A, Ceruti P, Gassino G, De Lillo A, Carossa S. Cephalometric evaluation of the upper airway in patients with complete dentures. Minerva Stomatol 2005;54:293-301.
20. Taner T, Saglam Aydintay B, Turkyilmaz I, Demir AU. The use of modified mandibular advancement appliance in the treatment of a partially edentulous patient with obstructive sleep apnea. Hacettepe Dishek Fak Derg 2007;31:82-7.
21. Giannasi LC, Magini M, Oliveira CS, Oliveira LV. Treatment of obstructive sleep apnea using an adjustable mandibular repositioning appliance fitted to a total prosthesis in a maxillary edentulous patient. Sleep Breath 2008;12:91-5.
22. Nayar S, Knox J. Management of obstructive sleep apnea in an edentulous patient with a mandibular advancement splint: a clinical report. J Prosthet Dent 2005;94:108-11.
23. Kurtulmus H, Cotert HS. Management of obstructive sleep apnea in an edentulous patient with a combination of mandibular advancement splint and tongue-retaining device: a clinical report. Sleep Breath 2009;13:97-102.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication March, 2014
Submitted in final revised form August, 2014
Accepted for publication August, 2014
Address correspondence to: Dr. Arvind Tripathi; MD 10, Sector C, Aliganj, Lucknow- 226024, Uttar Pradesh, India; E-mail: atrip2006@gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest. The work was performed at the Department of Prosthodontics, Saraswati Dental College & Hospital, Lucknow and Department of Pulmonary Medicine, King George’s Medical University, Lucknow, India. There was no off-label or investigational use.
PDF