Original Article 1, Issue 12.4
U.S. Army Obstructive Sleep Apnea and Oral Appliance Therapy Survey: A Qualitative Analysis of Comments
http://dx.doi.org/10.15331/jdsm.7408Christa E. Goodwin, DMD, MS1, Tyson L. Grier, MS2, Olivia M. Mahlmann, MPH2
1Tri-Service Center for Oral Health Studies, Uniformed Services University, Joint Base San Antonio – Fort Sam Houston, TX 78234, 2Defense Centers for Public Health – Aberdeen, APG, MD 21010
ABSTRACT
Objectives:
The purpose of this study is to describe U.S. Army soldiers’ comments regarding obstructive sleep apnea (OSA), including effects, diagnosis, and treatment.
Methods:
This is a secondary analysis of a subset of survey data received from a previous study that assessed soldiers’ self-reported impacts of OSA and the treatment oral appliance therapy (OAT). Comments provided in the survey’s text boxes were examined using an inductive approach to thematic analysis and organized into distinct, recurring categories.
Results:
Thirteen percent (n=1,131) of the 8,740 survey respondents provided comments; 6 categories and the most prevalent comments in each were identified. The most common positive OAT-related comment was the same as that of the positive airway pressure (PAP) device, which described overall satisfaction with the treatment, including improved sleep quality and/or quantity. The most common negative comment related to the PAP device described it as difficult to use and/or become habituated to; the most common negative OAT-related comment described the device as uncomfortable. Excessive daytime sleepiness was the most prevalent comment related to adverse effects of OSA, and the most common recommendation was that travel-sized PAP devices should be issued.
Conclusion:
Comments recounting effects of the disorder, relief (or no relief) from treatment, and adverse effects from treatment indicate OSA is a serious health concern compelling early diagnosis and improved treatment.
Clinical Implications:
Considering the number and nature of comments provided, an appraisal of the current military processes and procedures for screening, diagnosis, and treatment of soldiers suffering from OSA is justified.
Keywords:
obstructive sleep apnea; oral appliance therapy; Army; military; soldiers
Citation:
Goodwin C, Grier T, Mahlmann O. U.S. Army Obstructive Sleep Apnea and Oral Appliance Therapy Survey: A Qualitative Analysis of Comments. J Dent Sleep Med. 2025;12(4)
INTRODUCTION
Obstructive sleep apnea (OSA) is a highly prevalent and costly deployment-limiting sleep-related breathing disorder among U.S. Army soldiers.1–7 From 2014 through 2019, there were 87,404 cases of OSA diagnosed among this population;1 incidence rates ranged from 274.3 to 330.3 cases per 10,000 person-years.1 As of 2021, the prevalence of OSA among Army soldiers was estimated to be 12.15%.7
Sufficient sleep quality and duration are essential for deployment readiness and mission success. Poor sleep quality can result in an assortment of safety and health-related complications including increased risk of motor vehicle crashes, hypertension, cardiovascular disease, depression, and impaired cognitive and physical performance.8-10 Moreover, short sleep duration was found to be the strongest predictor of post-traumatic stress disorder among Army soldiers.11
Positive airway pressure (PAP) therapy remains the “gold-standard” treatment for OSA.12 However, considering military-specific characteristics (e.g., frequent traveling and deployments to austere locations with unreliable electricity), a PAP device is not always a practical treatment modality for soldiers. Additionally, a 2015 study concluded military service members diagnosed with OSA have low adherence to PAP therapy, as the majority (60.3%) of participants were found to be nonadherent.13 Oral appliance therapy is the leading alternative device to the PAP. This less cumbersome device is an effective treatment method for those suffering from mild to moderate OSA.1,14-18 The oral appliance has also demonstrated effectiveness for some patients with severe OSA who have not responded to or could not tolerate the PAP.17,18 Furthermore, studies have shown that many patients prefer the oral appliance to the PAP.16-18
The authors recently completed an OSA surveillance and oral appliance therapy evaluation among active duty U.S. Army soldiers.1,2 The purpose of the study was to determine the incidence of OSA among Army soldiers from 2014 through 2019 and to assess the self-reported impacts of the disorder and one of its treatments–oral appliance therapy. The self-reported data were obtained using an electronic survey. At the conclusion of the survey, respondents were provided with a text box giving them the opportunity to provide additional information about their experiences with OSA, including its effects, diagnosis, and treatment.1,2 This secondary analysis is a qualitative assessment of the comments soldiers provided.
Using text boxes in surveys is a way to gain valuable insight as respondents have the freedom to provide feedback in their own words. An additional method used to better understand patient perspectives is focus groups. This approach was tested in 2013 by Almeida et al. and 2016 by Luyster et al.; both studies evaluated patient experiences relating to OSA using a qualitative analysis of information gathered during focus group sessions.19,20 The aim of the 2013 study was to better understand patients’ perspectives and preferences about treatment with PAP therapy and the oral appliance.19 It concluded that a multitude of factors impact patients’ experiences with treatment, and that their treatment needs are not just physical but lifestyle-related as well.19 The 2016 study evaluated patient and partner experiences with OSA and PAP therapy, both of who underscored the value of partner involvement in the early treatment period.20 The results of the study recommended that future adherence interventions follow a couples-oriented approach to improving PAP therapy adherence.20
The 2013 and 2016 qualitative assessments captured very meaningful information regarding patient perspectives, preferences, and ideas as they relate to OSA. However, they were civilian-based studies. A 2024 military-based pilot study compared soldier preference between 2 types of oral appliances for treating OSA and bruxism.21 The qualitative aspect of this study consisted of both phone and in-person consultations used to determine tolerability, compliance, and preference; the modified ProSomnus IATM was determined to be the preferred device for most patients.21 While this 2024 study compared only 2 types of oral appliances (ProSomnus IATM and TAP 3TM) in a very small cohort (n=13), its findings emphasize the value of acknowledging patient perspectives and preferences when determining the best course of treatment.21
The current study is not the first military-based qualitative analysis of comments relating to the treatment of OSA. However, considering the number, length, and relevance of comments soldiers provided in this survey, a thorough evaluation is warranted. Therefore, the purpose of this secondary analysis is to better understand Army soldiers’ perspectives and experiences regarding OSA, including diagnosis, effects, and treatments.
METHODS
This qualitative investigation is a secondary analysis of a larger, previously completed study.1,2 Respondents’ comments in the survey’s text boxes were thoroughly examined; no other information collected from the survey was used in this assessment. This investigation was approved by the Defense Centers for Public Health – Aberdeen (formerly the U.S. Army Public Health Center) Public Health Review Board (#19-744).
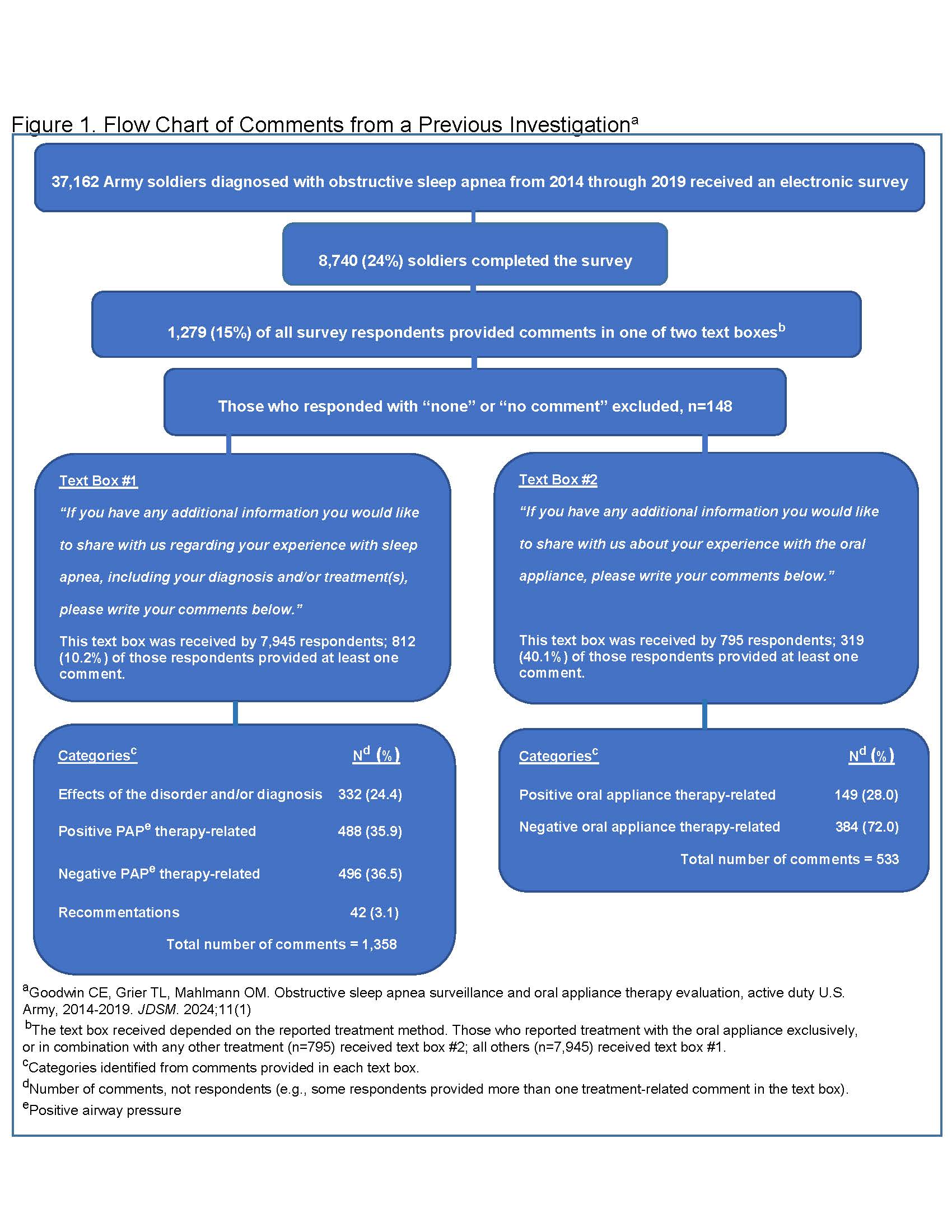
Respondents were asked to report their current OSA treatment method(s) in the survey. Considering treatment for OSA is commonly multidisciplinary, respondents had the option of selecting more than one treatment method (e.g., oral appliance therapy, PAP therapy, lifestyle changes, other, and no treatment). At the close of the survey, respondents were prompted with one of two text boxes giving them the opportunity to provide additional information. The text box each respondent received depended on the reported treatment method (Figure 1). Those who reported treatment with anything other than an oral appliance were prompted with the following open-ended statement above the text box: “If you have any additional information you would like to share with us regarding your experience with sleep apnea, including your diagnosis and/or treatment(s), please write your comments below.” Those who reported treatment with an oral appliance, either exclusively or in combination with any other method, received the following open-ended statement above the text box: “If you have any additional information you would like to share with us about your experience with the oral appliance, please write your comments below.” For the purposes of this analysis, when soldiers provided very lengthy responses touching on more than one subject (e.g., some soldiers provided both diagnosis and treatment-related comments in the text box) these were treated as separate comments. Those who responded with comments such as “none,” “N/A,” or “no comment” were excluded (n=148).
A thematic-based analysis with an inductive approach was chosen as this is a successful technique for identifying common topics, ideas, and patterns within qualitative data.22 An inductive method allows the data to determine the themes as opposed to approaching the data with predetermined themes (i.e., deductive method). A software package was not used in this analysis. The primary author thoroughly reviewed all comments and generated an initial set of codes (i.e., brief description of each comment). The initial set of codes was reviewed again after which some were appropriately modified. Similar codes were then grouped together until broader patterns and themes were identified; each theme was given a distinct name. At this point the second author reviewed all comments, codes, and themes. Any disagreements were discussed, and a final decision was reached. Themes ultimately derived were further labeled as “categories” and are presented below, as are the most frequent comments in each of these categories.
RESULTS
Of the 8,740 soldiers who responded to the survey, 15% (n=1,279) provided comments in the text boxes; 148 were excluded for providing responses such as “none” or “no comment.” Therefore, responses from 1,131 soldiers were included in the final analyses resulting in a total of 1,891 individual comments. Figure 1 provides a flow chart detailing the number of comments received in each text box (labeled text box #1 and text box #2) as well as the 6 identified categories which include the following: 1. Effects of the disorder and/or diagnosis; 2. Positive PAP therapy comments; 3. Negative PAP therapy comments; 4. Recommendations; 5. Positive oral appliance comments; 6. Negative oral appliance comments. Categories 1 through 4 were derived from the comments provided in text box #1; categories 5 and 6 were derived from text box #2.
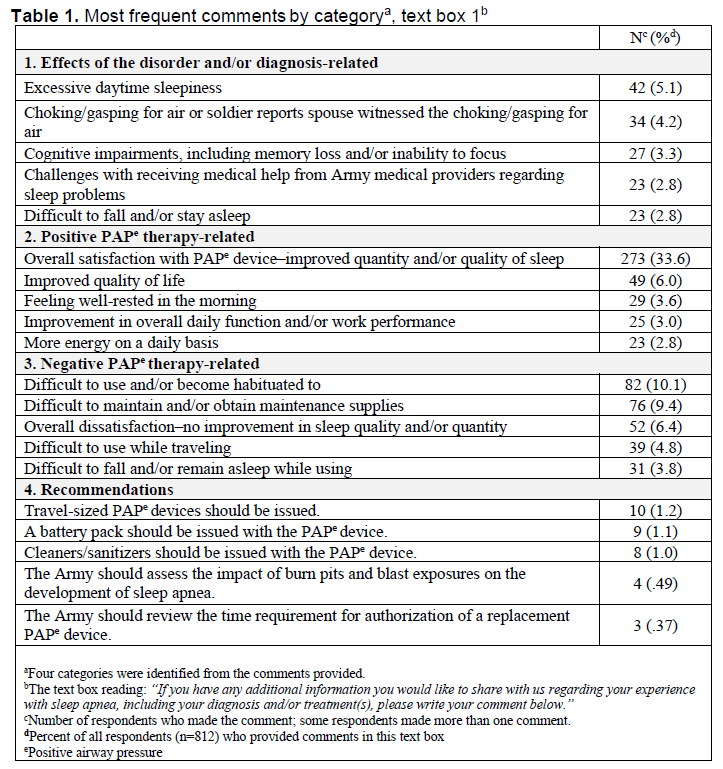
Text box #1 inquired about experiences with OSA and was received by 7,945 respondents; 812 (or 10.2%) of those respondents provided at least one comment for a total of 1,358 comments. The number and percent of comments in each category included the following: effects of the disorder and/or diagnosis (n=332 or 24.4%), positive PAP therapy-related (n=488 or 35.9%), negative PAP therapy-related (n=496 or 36.5%), and recommendations (n=42 or 3.1%) (Figure 1). Table 1 lists the most frequent comments in each of these 4 categories.
The most prevalent comment relating to the effects of the disorder and/or its diagnosis, reported by 5.1% (n=42) of respondents, was excessive daytime sleepiness. Other frequent comments included choking/gasping for air during the night (or the spouse witnessed the choking/gasping), cognitive impairments, including memory loss and/or the inability to focus, challenges receiving help from providers regarding sleep disturbances, and difficulty falling and/or staying asleep (Table 1).
The most common positive PAP therapy-related comment, reported by 33.6% (n=273) of respondents, described overall satisfaction with the device, including improved sleep quality and/or quantity. Other common positive comments included improved quality of life, feeling well-rested in the morning, improvement in overall daily function and/or work performance, and more energy daily (Table 1).
The most common negative PAP therapy-related comment, reported by 10.1% (n=82) of respondents, described the device as difficult to use or become habituated to. Other frequent negative comments included maintenance difficulty, overall dissatisfaction (i.e., no improvement in sleep quality and/or quantity), difficult to use while traveling, and difficult to fall and/or remain asleep while using. The most common recommendation, provided by 10 respondents (1.2%), was that travel-sized PAP devices should be provided by the military (Table 1).
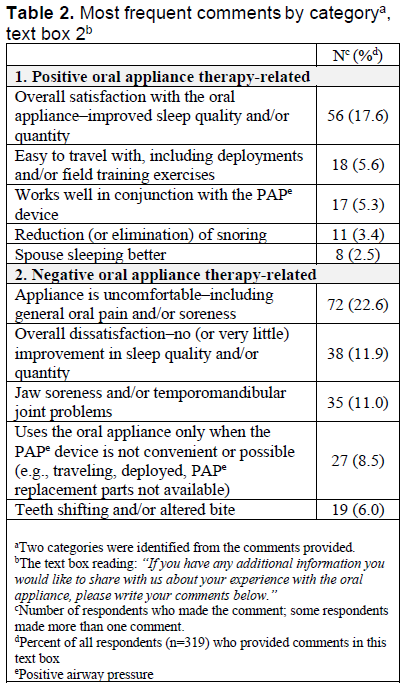
Text box #2 inquired about the oral appliance and was received by 795 respondents; 319 (or 40.1%) of those respondents provided at least one comment for a total of 533 comments (Figure 1). The majority of comments fell into one of two categories–positive or negative oral appliance therapy-related. While some respondents had only positive or negative things to report about this treatment method, other respondents provided both positive and negative feedback. In total there were 149 (or 28.0%) positive oral appliance-related comments and 384 (or 72.0%) negative oral appliance-related comments (Figure 1).
Table 2 lists the most frequent comments in each of these 2 categories. The most common positive comment, reported by 17.6% (n=56) of respondents, described overall satisfaction with the appliance, including improved sleep quality and/or quantity. Other common positive comments described the appliance as easy to travel with, works well in conjunction with the PAP device, reduces (or eliminates) snoring, and improved sleep for the spouse.
The most common negative oral appliance comment, reported by 22.6% (n=72) of respondents, described the appliance as uncomfortable, including general oral pain and/or soreness. Other common negative comments included overall dissatisfaction, with no (or very little) improvement in sleep quality and/or quality, jaw soreness, use of the appliance only when the PAP device is not convenient (e.g., during travel or deployment), and teeth shifting and/or altered bite (Table 2).
Figure 1. Flow Chart of Comments from a Previous Investigationa |
{kind=link}
Table 1. Most frequent comments by categorya, text box 1b
{kind=link}
Table 2. Most frequent comments by categorya, text box 2b
{kind=link}
DISCUSSION
This study evaluated U.S. Army soldiers’ comments regarding OSA using an inductive approach to thematic analysis. Categories among the comments were identified including positive and negative treatment-related comments, effects of the disorder and/or diagnosis, and recommendations. The most prevalent comments in each category were presented.
Thirteen percent of soldiers who completed this survey took time to provide comments sharing their experiences with OSA including effects, diagnosis, and treatment(s). Many of the comments were lengthy, suggesting these soldiers were very eager to express their thoughts regarding OSA, its impact on them and/or their significant others, the diagnostic process, successes or failures with treatment, and side effects of treatment.
The number of those who completed the OSA text box (text box #1) was 2.5 times the number of those who completed the oral appliance text box (text box #2). This was not surprising as the OSA text box was received by 10 times as many respondents. However, it was interesting to find that the proportion of respondents who completed the oral appliance text box was 4 times greater than that of those who completed the OSA text box. This finding might be explained by the number and nature of the comments. There were a similar number of negative and positive PAP-related comments in the OSA text box. However, there were over twice as many negative oral appliance comments compared to positive. This was unexpected given that in the initial study soldiers treated with the oral appliance reported statistically significant improvements in sleep quality, duration, alertness, cognition, and various other aspects of daily life.1,2 It could be suggested that the greater number of negative oral appliance comments in relation to positive found in this secondary analysis is not a reflection of the oral appliance’s ability (or lack thereof) to successfully treat patients with OSA. Instead, those who had negative experiences with the oral appliance may have been impacted on a deeper level than those who had positive experiences, and thus, were more inclined to provide additional comments. This type of bias, also known as the negativity effect, is the proclivity to not only register negative stimuli more readily than positive, but to focus more attention on them as well.23,24
The most common negative oral appliance-related comment described the appliance as uncomfortable with no improvement in sleep quality and/or quantity. Other common negative remarks detailed the various adverse effects from the appliance. A 2021 systematic review and meta-analysis investigated the factors influencing adherence to oral appliance therapy in adults diagnosed with OSA;25 31 studies were included in this analysis, all of which took place in academic medical or sleep centers. The factors found to influence adherence to the oral appliance were very similar to the negative comments provided in our survey. Nonadherence, or early discontinuation of treatment, was recognized due to side effects including dental pain and muscular pain, as well as overall inefficacy of the treatment.25 The most common self-reported explanation for nonadherence was “lack of treatment effect or discomfort or pain” associated with use of the oral appliance.25
The 2024 military-based pilot study discussed earlier compared soldier preference between 2 types of oral appliances for the treatment of OSA and bruxism.21 Overall, the ProSomnus IATM was preferred by soldiers given its smooth material, comfort, and ease of placement.21 However, a reason given for preference of the TAP 3TM over the ProSomnus IATM included discomfort in the cheeks when using the ProSomnus IATM in conjunction with the PAP.21 While discomfort was one of the most common negative oral appliance-related comments provided by soldiers in the current study, a distinct difference between the 2024 study and this study must be underscored. The authors did not determine which specific oral appliances soldiers were treated with, if they used the PAP in conjunction with the oral appliance, or if they were also diagnosed with sleep bruxism. These are all factors that can significantly impact patient satisfaction, preference, compliance, and ultimately efficacy of treatment. Furthermore, continuity of care following delivery of an oral appliance is paramount to confirming efficacy of the treatment and addressing any possible adverse effects, both of which can impact compliance. Therefore, it is important to recognize characteristics specific to the military that make continuity of care a challenge (e.g., soldiers, including health care providers, change duty stations every 2 to 3 years). Consequently, insufficient continuity of care may have contributed to the dissatisfaction expressed by soldiers in this survey. However, that cannot be confirmed as the authors did not examine soldiers’ medical/dental treatment records. Certainly, more research evaluating oral appliance satisfaction, preference, and compliance among Army soldiers is warranted.
The most prevalent negative PAP-related comments described various difficulties associated with the device—difficult to habituate to, to travel with, to remain asleep with, and to maintain. A 2020 study investigated the factors impacting patients’ adherence to the PAP device.26 Part of this study included a qualitative analysis performed through telephone interviews with patients previously determined to be nonadherent to the PAP.26 The analysis resulted in 3 categories that contributed to nonadherence including knowledge, problems/discomfort, and costs.26 These categories were further broken down into subcategories, several of which were very similar to the negative comments received in our survey (e.g., the PAP is difficult to use while traveling, device problems and discomfort making use difficult, and lack of knowledge regarding maintenance).26
Soldiers provided comments regarding the effects of the disorder, the most common being excessive daytime sleepiness, choking/gasping for air, and cognitive impairments. These remarks are consistent with the OSA clinical signs and symptoms established by the medical community.8 Furthermore, it is believed that nocturnal choking/gasping for air “may be the most useful individual complaint suggesting OSA.”8
LIMITATIONS
A distinct limitation to this study is that the material it is founded on is purely subjective; these types of anecdotal records cannot be confirmed. However, considering the quantity of comprehensive comments, as well as the many similarities among them, these remarks are assuredly relevant and should be sincerely appreciated. An additional limitation specific to using self-reported data includes the introduction of unintentional biases. Nevertheless, the use of text boxes provides valuable insights that may be missed with the use of closed-ended survey items. Furthermore, considering the unique characteristics of the military population and profession (e.g., younger average age and greater proportion of men compared to the general population, changing of duty stations every 2 to 3 years, deployments to austere locations, frequent traveling, etc.) the results of this study may not necessarily be transferable to the general population.CONCLUSIONS
The positive comments describing improved sleep quality and/or quantity following treatment suggest both the oral appliance and PAP device are effective treatment modalities for U.S. Army soldiers. However, considering the number of negative treatment-related comments, it is evident that the same treatment that is successful for one soldier may be unsuccessful for another. Comments depicting challenges with receiving a diagnosis and effective treatment suggest there are some obstacles within the military health care system. Comments recounting adverse effects of the disorder (e.g., excessive daytime sleepiness, inability to focus, diminished physical ability, etc.) indicate OSA is a serious health concern compelling early diagnosis and treatment. Untreated OSA can have substantial implications on soldiers’ health, deployment readiness, mission performance, and overall mission success. Considering the number and nature of comments provided in this survey, an appraisal of the current processes and procedures for screening, diagnosis, and management of soldiers suffering from OSA is justified.
ABBREVIATIONS
OSA – obstructive sleep apnea
OAT – oral appliance therapy
PAP – positive airway pressure
REFERENCES
1. Goodwin C, Grier T, Mahlmann O. Obstructive sleep apnea surveillance and oral appliance therapy evaluation, active duty US Army, 2014-2019. J Dent Sleep Med. 2024;11(1).2. Goodwin C, Grier T, Mahlmann O. Obstructive sleep apnea surveillance and oral appliance therapy evaluation, active duty US Army, 2014-2019. U.S. Army Public Health Center Technical Report No. S.0079064.3-21. May 2022. https://apps.dtic.mil/sti/pdfs/AD1171341.pdf
3. Rogers A, Stahlman S, Hunt D, Oh G, Clark L. Obstructive sleep apnea and associated attrition, active component, U.S. armed forces, January 2004-May 2016. MSMR. 2016; 23(10): 2-11.
4. Health of the Force Report (2022). Defense Centers for Public Health-Aberdeen. Defense Health Agency. https://ph.health.mil/Periodical%20Library/2022-hof-report.pdf#search=health%20of%20the%20force. Accessed 25 April 2025.
5. Knowles S, Dekow M, Williamson M. Oral appliances for OSA treatment: meeting the Quadruple Aim. Mil Med.2023;188(3-4):e718-e724. https://doi.org/10.1093/milmed/usab316
6. United States Central Command. USCENTCOM. Modification Seventeen (Tab A): Amplification of the Minimal Standards of Fitness for Deployment to the CENTCOM AOR; to Accompany Modification Seventeen to USCENTCOM Individual Protection and Individual/Unit Deployment Policy. https://www.centcom.mil/Portals/6/MEDICAL/MOD17_Tab_A.pdf. Accessed 25 April 2025.
7. Haynes Z, Stewart I, Poltavskiy E, et al. Obstructive sleep apnea among survivors of combat-related traumatic injury: a retrospective cohort study. J Clin Sleep Med. 2022;18(1):171–179.
8. Kryger M, Roth T, Goldstein C, Dement W. Principles and Practice of Sleep Medicine. 7th edition. Elsevier; 2022.
9. Gottlieb D, Punjabi N. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389-1400.
10. Sateia M. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387-1394. https://doi.org/10.1378/chest.14-0970.
11. Walter Reed Army Institute of Research. Comprehensive Fatigue Management: Maintaining Cognitive Dominance and the Tactical Advantage in Multi-Domain Operations. 26 July 2023. https://media.defense.gov/2023/Jul/26/2003268441/-1/-1/1/COMPREHENSIVE-FATIGUE-MGMT-RELEVANCE-DOC-WRAIR-V1.PDF. Accessed 25 April 2025.
12. Patil S, Ayappa I, Caples S, et al. Treatment of adult obstructive sleep apnea with positive airway pressure: an American Academy of Clinical Practice Guideline. JCSM. 2019;15(2):335-343.
13. Mysliwiec V, Capaldi F, Gill J, et al. Adherence to positive airway pressure therapy in U.S. military personnel with sleep apnea improves sleepiness, sleep quality, and depressive symptoms. Mil Med. 2015;180(4):475-482.
14. Lettieri C, Paolino N, Eliasson A, et al. Comparison of adjustable and fixed oral appliances for the treatment of obstructive sleep apnea. J Clin Sleep Med. 2011;7(5):439-445.
15. Lim J, Lasserson T, Fleetham J, Wright J. Oral appliances for obstructive sleep apnea. Cochrane Database Syst Rev.2006;25(1):CD004435.
16. Sutherland K, Phillips C, Cistulli P. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. J Dent Sleep Med. 2015;2(4):175-181.
17. Phillips C, Grunstein R, Darendeliler M, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: A randomized controlled trial. Am J Respir Crit Care Med.2013;187(8):879-887.
18. Doff M, Hoekema A, Wijkstra P, et al. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: a 2-year follow-up. Sleep. 2013;36(9):1289-96. https://doi.org/10.5665/sleep.2948.
19. Almeida F, Henrich N, Marra C, et al. Patient preferences and experiences of CPAP and oral appliances for the treatment of obstructive sleep apnea: a qualitative analysis. Sleep Breath. 2013 May;17(2):659-66. doi: 10.1007/s11325-012-0739-6. Epub 2012 Jul 26. PMID: 22833346.
20. Luyster F, Dunbar-Jacob J, Aloia M, et al. Patient and partner experiences with obstructive sleep apnea and CPAP treatment: A qualitative analysis. Behav Sleep Med. 2016;14(1):67-84. doi: 10.1080/15402002.2014.946597. Epub 2014 Sep 9. PMID: 25203283; PMCID: PMC4363003.
21. Ryser A, Sabol J, Handel S, Walworth P, Dimalanta W, et al. Soldier preference in mandibular advancement devices in patients who brux. J Dent Oral Epidemiol. 2024;4(2): doi https://doi.org/10.54289/JDOE2400110
22. Jones, S. Interpreting themes from qualitative data: thematic analysis. Eval Academy. February 2022. https://www.evalacademy.com/articles/interpreting-themes-from-qualitative-data-thematic-analysis. Accessed 25 April 2025.
23. Haizlip J, May N, Schorling J, et al. Perspective: the negativity bias, medical education, and the culture of academic medicine. Acad Med.2012;87(9):1205-1209. https://doi.org/10.1097/ACM.0b013e3182628f03.
24. Baumeister R, Bratslavsky E, Finkenauer C, et al. Bad is stronger than good. Rev Gen Psychol. 2001;5:323–370.
25. Tallamraju H, Newton J, Fleming P, et al. Factors influencing adherence to oral appliance therapy in adults with obstructive sleep apnea: a systematic review and meta-analysis. J Clin Sleep Med. 2021;17(7):1485-1498. https://doi.org/10.5664/jcsm.9184.
26. Aalaei S, Rezaeitalab F, Tabesh H, et al. Factors affecting patients' adherence to continuous positive airway pressure therapy for obstructive sleep apnea disorder: a multi-method approach. Iran J Med Sci.2020;45(3):170-178. https://doi.org/10.30476/ijms.2019.45785.27.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted February 26, 2025
Submitted in final revised form May 12, 2025
Accepted for publication July 7, 2025
Address correspondence to: LTC Christa E. Goodwin, DMD, MS. Email: christa.goodwin@usuhs.edu
DISCLOSURE STATEMENT
The opinions and assertions expressed herein are those of the authors and do not reflect the official policy or position of the Uniformed Services University of the Health Sciences, Department of the Army, Department of Defense, or U.S. Government.References to non-Federal entities or products do not constitute or imply a Department of Defense or Uniformed Services University of the Health Sciences endorsement.
The authors do not have a financial interest in any commercial product, service, or organization providing financial support for this research.
All authors declare no conflict of interest
This protocol was reviewed and approved by the Defense Centers for Public Health – Aberdeen Public Health Review Board (#19-744).