Original Article 1, Issue 12.3
US Military Dental Providers’ Knowledge, Attitudes, and Practice Behaviors Relating to Obstructive Sleep Apnea and Oral Appliance Therapy
http://dx.doi.org/10.15331/jdsm.7400Christa E. Goodwin, DMD, MS1
1Director, Tri-Service Center for Oral Health Studies, Uniformed Services University of the Health Sciences, Joint Base San Antonio – Fort Sam Houston, TX 78234
ABSTRACT
Objectives:
This study assessed the knowledge, attitudes, and practice behaviors of active-duty Army, Air Force, and Navy dentists regarding obstructive sleep apnea (OSA) and oral appliance therapy.
Methods:
An electronic survey was distributed via email to active-duty military dentists. The main component of this survey included the validated 24-item questionnaire - Obstructive Sleep Apnea Knowledge and Attitudes (OSAKA) questionnaire, consisting of 18 true-false knowledge items and 6 Likert scale attitude items; additional survey items not associated with OSAKA inquired about oral appliance therapy practice behaviors.
Results:
A total of 337 military dentists (Army = 76; Navy = 108; Air Force = 151) completed the survey. Scores for all dentists overall ranged from 1 to 18 with a mean knowledge score of 14.6 or 81.1%. There were no statistically significant differences in the knowledge scores of military dentists by service, sex, age group, advanced training, or specialty training. There was a statistically significant positive correlation between age and 2 attitude items pertaining to confidence; as age increased, so did reported confidence in the ability to recognize (P = .007) and manage (P < .001) adverse effects from the oral appliance.
Conclusion:
Expanding the number of military health care providers screening for and managing OSA patients can help address the health care concern of undiagnosed and untreated OSA in the military; results of this study suggest military dentists can and should be engaged in this effort.
Clinical Implications:
Including military dentists in the multidisciplinary approach of diagnosing and managing OSA patients will improve the health of service members, thereby advancing combat readiness, mission success, and the military as a whole.
Keywords:
military; dentists; obstructive sleep apnea; oral appliance therapy
Citation:
Goodwin C. US Military Dental Providers’ Knowledge, Attitudes, and Practice Behaviors Relating to Obstructive Sleep Apnea and Oral Appliance Therapy. J Dent Sleep Med. 2025;12(3)
INTRODUCTION
Obstructive sleep apnea (OSA), the most common sleep-related breathing disorder, is highly prevalent among the US military population and associated with expanding economic- and health-related burdens.1-13 The military population is generally known to be healthy, young, and physically fit. Nonetheless, the rates of OSA have continued to rise over the last two decades. Between 2000 and 2009, there was a remarkable 6-fold increase in incident diagnoses of OSA among active-duty military service members.2 The increase was nearly 8-fold during this 10 year period for those over 40 years old.2 From 2009 through 2015, there were 170,604 incident cases of OSA identified among service members; incidence rates ranged from 138 to 202.4 cases per 10,000 person-years.3 A more recent study evaluated OSA diagnoses among active-duty service members from 2005 through 2019.4 Overall there were 393,857 new cases of OSA diagnosed; incidence rates ranged from 11.8 to 333.8 cases per 10,000 service members.4 Those diagnosed most often during this period were White (61%), male (92%), in the Army (48%), and 40 years of age or older (39%).4 As of 2021, the prevalence of OSA among military service members was estimated to be the highest among the Army (12.15%), followed by the Air Force (9.96%), and finally the Navy (9.06%).5
OSA diagnoses among military service members generate substantial costs to both the Department of Defense as well as the Department of Veterans Affairs. Expenses associated with a service member’s OSA diagnosis include treatment-related costs of both OSA and connected adverse health conditions, as well as military disability benefits upon separation or retirement from service.12-13 The assigned disability rating can vary; a diagnosis of OSA requiring the use of a positive airway pressure (PAP) device provides a 50% disability rating.12 According to the 2025 disability compensation rates, a veteran with a 50% disability rating is entitled to a compensation of $1,102 per month.13
Quality sleep is integral for service members’ deployment readiness and mission performance. Poor sleep quality is connected to a myriad of health- and safety-related complications such as excessive daytime sleepiness, depression, increased risk of motor vehicle accidents, arrhythmias, stroke, impaired cognition, respiratory abnormalities, diabetes, and cardiovascular disease.14-17 Furthermore, the strongest predictor of post-traumatic stress disorder among Army soldiers is short sleep duration.17
Unfortunately, OSA is a disorder that often remains undiagnosed and, thus, untreated.15,18,19 According to the American Academy of Sleep Medicine (AASM), approximately 80% of adult Americans with OSA remain undiagnosed.19 Untreated OSA among the military population, particularly, is a serious concern considering the inherent characteristics, operational demands, responsibilities, and overall function of the profession. Service members must preserve vigilance under a variety of circumstances and in austere environments; they are required to make quick, critical decisions. Poor sleep quality and duration can negatively impact their cognition, alertness, motor function, physical performance, and overall performance.1,6,17,20 A 2022 study tested sleep as a possible factor impacting the performance of Army infantry soldiers during battle drill training.20 Subjective sleep items included self-reported sleep duration (hours of total sleep time) and quality (sleep efficiency out of 100). An objective measure of the sleep/wake cycle was also captured with the use of an actigraph.20 Soldiers performed infantry battle drill training in the form of close-quarters battle drills; the number of errors committed during the drills was recorded. Soldiers who received greater than or equal to 7 hours of sleep had a significantly lower number of errors compared to those who received less than 7 hours of sleep.20 Furthermore, those who reported a sleep quality of less than 85% committed more errors than those with sleep quality of greater than or equal to 85%.20
A PAP device remains the gold-standard treatment for OSA. However, compliance is low and its use is not practical in forward-deployed environments.21,22 Oral appliance therapy is an effective treatment for those diagnosed with mild to moderate OSA.1,23,24 Results of a recent study demonstrate Army soldiers are satisfied with this treatment; oral appliance therapy significantly improved their sleep quality and duration, as well as other aspects of daily life including physical activity, alertness, performance, and cognition.1 Given its ease of use compared to PAP devices, an oral appliance can be regarded as a ‘simpler’ therapeutic option—a noteworthy point considering the nature of the military profession (e.g., deployments to austere locations with unreliable electricity). Dentists trained in dental sleep medicine (DSM) are currently the only providers with the knowledge and expertise to provide oral appliance therapy.25,26 DSM is an extension of general dentistry; it is not considered a dental specialty. DSM dentists have the training to screen patients for OSA, collaborate with other health care providers regarding diagnosis and treatment options, educate patients, initiate oral appliance therapy, manage adverse effects, and provide follow-up care, as needed.26
Diagnosis of OSA is reserved for physicians; dentists are not qualified to diagnose this disorder. However, they are in a unique position to assist in identifying those at risk of OSA. Military dentists, specifically, have an advantage because service members are required to undergo a yearly dental exam that provides dentists with the opportunity to evaluate these individuals for oral and facial anatomic characteristics considered risk factors for OSA and other sleep-related breathing disorders (e.g., large neck circumference, retrognathia, pharyngeal crowding, macroglossia, sleep bruxism, enamel erosion).25-28 Moreover, the recommendations and position statements of medical and dental associations including the American Dental Association and the AASM agree a dentist’s role includes screening patients for OSA and referring to sleep medicine physicians when OSA is suspected.25-28 Unfortunately, not all dentists are trained to recognize OSA risk factors or manage OSA patients with oral appliance therapy. The amount of education regarding sleep medicine dentists receive in a dental school doctorate program is minimal.
A questionnaire assessing the knowledge and attitudes of physicians regarding OSA was developed and validated in 2003.29 The Obstructive Sleep Apnea Knowledge and Attitudes (OSAKA) questionnaire is a 23-item tool consisting of 18 true-false knowledge statements and 5 Likert scale attitude statements. The knowledge items are distributed among 5 OSA-related domains including epidemiology, pathophysiology, symptoms, diagnosis, and treatment. The attitude items allow respondents to attribute a level of importance to OSA-related statements and rate their level of confidence in their ability to perform OSA management-related tasks.29
The OSAKA was determined to be a suitable instrument for measuring the knowledge and attitudes of physicians regarding OSA.29 This tool has since been employed in subsequent studies, not just among physicians but dentists as well. A 2021 study used the OSAKA to determine whether California dentists were as knowledgeable about this disorder as US and non-US physicians of various specialties (e.g., cardiology, internal medicine, otolaryngology, anesthesiology, pediatrics, etc.).30 The total knowledge score of California dentists (n=170) was compared to a collection of published knowledge scores of physicians from 12 studies carried out during the years 2003 through 2020.30 Dentists had a mean total knowledge score of 73.6%. The mean score of all US and non-US physicians (n=2,559) was 63.9%; the score for US physicians (n=305) was 75.6%. The group with the highest mean knowledge score (84.5%) was Canadian otolaryngology residents (n=66). Ultimately, dentists’ OSA knowledge was determined to be noninferior to that of most physician groups.30
Military dentistry is poised to advance military medicine. Expanding the role of military dentists to include screening for OSA, referral, and management, when appropriate, is a valuable first step to addressing the health care concern of undiagnosed and untreated OSA in the military. Collaboration between dentists and physicians can synergize the OSA diagnostic and treatment processes. However, this cannot be accomplished without first evaluating the baseline knowledge of military dentists regarding OSA. Identifying shortcomings in this area will facilitate developing OSA- and oral appliance therapy-related educational interventions targeted specifically for military dentists. Therefore, the purpose of this study is to assess the knowledge, attitudes, and practice behaviors of active-duty Army, Air Force, and Navy dentists regarding OSA and oral appliance therapy.
METHODS
This study protocol was reviewed and approved by the Uniformed Services University Human Research Protection Program; it was assigned number DBS.2023.540 and determined to be an exempt protocol under the provision of 32 CFR 219.104(d)(2)(i). All data were obtained from an electronic survey created using Survey Monkey. The main component of this survey consisted of the OSAKA questionnaire, copyright by Washington University in St Louis, Missouri, used with permission.29 Distribution of this survey also required approval from the Defense Health Agency (DHA); the survey was assigned DHA Survey Control Number: DHA-1088.
At the time this study took place, there were 2,926 active-duty military dentists (Army = 967, Air Force = 853, Navy = 1,106). The original intent was to distribute the survey to all Army, Air Force, and Navy dentists. However, this proved to be an impractical goal as email distribution lists for all military dentists are not readily available. When select leaders from each service were contacted, a piecemeal approach to distribution was offered and ultimately executed. This approach included disseminating the survey link via email to the various regional dental commanders/leaders from each service, then down to the dental leaders serving under those commanders, and so on, until it (ideally) reached the dentists serving at each military installation. The survey link was also posted in the Navy Weekly Dental Update for several weeks. This is a weekly electronic bulletin produced by and for the Navy Dental Corps. The survey opened in June 2023 and closed in November 2023.
The OSAKA knowledge and attitude items were embedded within a larger survey. Respondents were initially asked an exclusion question; the survey immediately ended for those who selected the response that indicted they were not currently an active-duty military dentist. Next, respondents were asked to answer various demographic questions identifying their service (Army, Air Force, or Navy), sex, age group, and type of advanced and/or specialty training, if applicable. Currently there are 12 dental specialties formally recognized by the National Commission on Recognition of Dental Specialties and Certifying Boards (e.g., endodontics, prosthodontics, periodontics, etc.); however, the military also recognizes a thirteenth specialty known as comprehensive dentistry. Advanced training refers to either an Advanced Education in General Dentistry (AEGD) or General Practice Residency (GPR). Both a GPR and AEGD are optional one-year programs designed to improve and refine a dentist’s knowledge and clinical skills in the practice of general dentistry, the main difference being that a GPR is a hospital-based program.
The OSAKA items followed the demographic questions. This study used the dental version of OSAKA. There were 18 true-false knowledge items, one of which pertained to oral appliance therapy. “Don’t know” was included as a third response to minimize guessing; “don’t know” responses were scored as incorrect. Six attitude items followed. The first 2 items asked respondents to rate the importance of OSA as a clinical disorder and the importance of identifying patients with OSA. The next 4 items asked respondents to rate their confidence levels, including confidence in their ability to identify those at risk of OSA, manage patients with OSA using the oral appliance, recognize possible adverse effects from the oral appliance, and manage adverse effects of the oral appliance.
Once respondents completed the OSAKA questionnaire, they were asked if they were currently practicing DSM (i.e., had the necessary training, credentials, and privileges to manage OSA patients with the oral appliance). The survey immediately ended for those who selected “No.” Those who selected “Yes” were prompted with additional items regarding their oral appliance therapy practice behaviors. In the final section of the survey, DSM dentists were asked about years in practice followed by perceived level of expertise. Subsequent items covered practice behavior specifics such as the number of appliances delivered per month, observed adverse effects, and management of adverse effects.
Survey data were analyzed using Microsoft Excel and IBM SPSS Statistics 29.0.2.0 (20). The main outcome variables included knowledge and attitudes. A total knowledge score was calculated for each respondent; scores could range from 0 to 18. Attitudes were represented by 2 importance and 4 confidence-related items, each measured on a 5-point Likert scale, with “1” representing the lowest level of importance (or confidence) and “5” representing the highest level of importance (or confidence). Perceived level of expertise was also an outcome variable, though this variable only pertained to DSM dentists; it was measured with one 5-point Likert scale item (1-novice, 5-expert). In-dependent variables included sex, age group, service, advanced training, and specialty training. Shapiro-Wilk normality tests indicated the data were not normally distributed. Thus, nonparametric tests were used for subsequent bivariate analysis of the survey data. Correlations between knowledge and attitudes were measured using the Kendall τ (tau) rank correlation test. Mann-Whitney U tests were used to evaluate the differences in the outcome variables by sex, advanced training, and specialty training. The specialty training variable used in this analysis was a categorical Yes/No variable (i.e., 2 groups - those who have and those who have not completed specialty training). Differences in the outcome variables by service were evaluated using Kruskal-Wallis-H tests. Differences in knowledge and attitudes by individual specialty and service (e.g., knowledge/attitudes of Army prosthodontists compared to that of Navy and Air Force prosthodontists) were not evaluated due to the very small sizes of the individual specialty groups in each service.
RESULTS
Survey Respondent Demographics
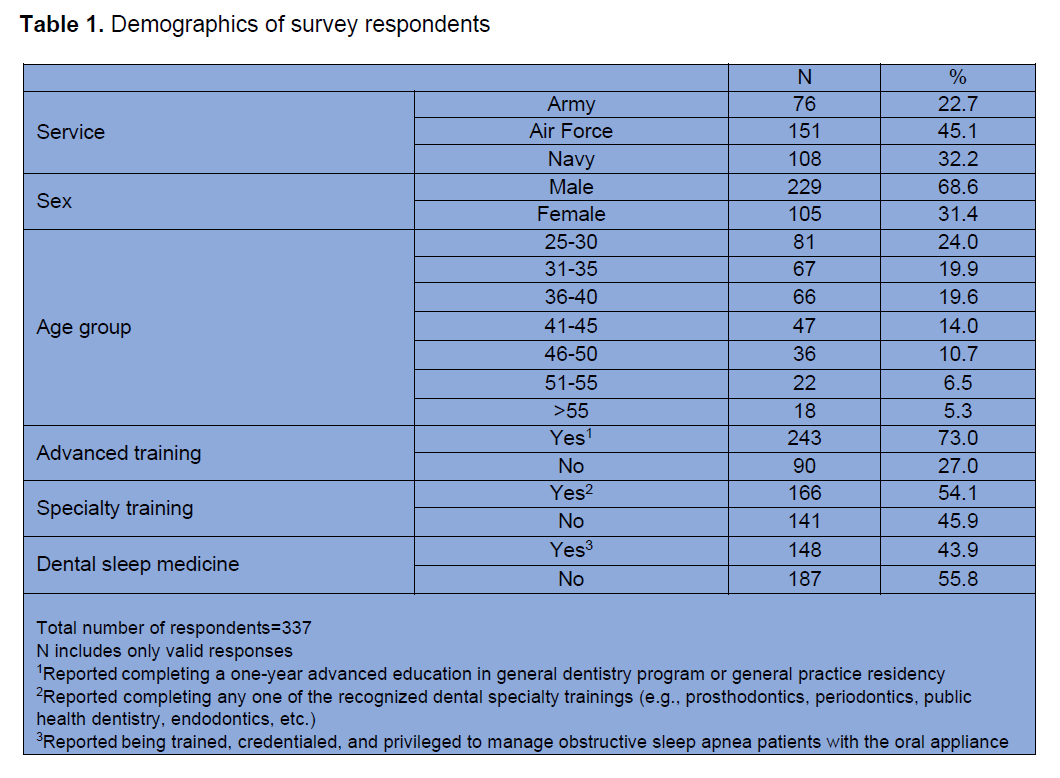
The survey was initiated by 387 military dentists, though not all completed it in its entirety. Only those who completed all 18 knowledge and 6 attitude items in the OSAKA section (n=337) were included in the final analyses. Table 1 displays the demographics of survey respondents. Almost half (45.1%, n=151) were Air Force dentists, 32.2% (n=108) were Navy, and the Army represented the smallest proportion (22.7%, n=76) of respondents. The majority (68.6%, n=229) of respondents were male; 31.4% (n=105) were female. Dentists 25 to 30 years of age represented the largest proportion of respondents (24%, n=81); those 31 to 35 years of age represented 19.9% (n=67) as did those 36 to 40 years of age (19.6%, n=66).
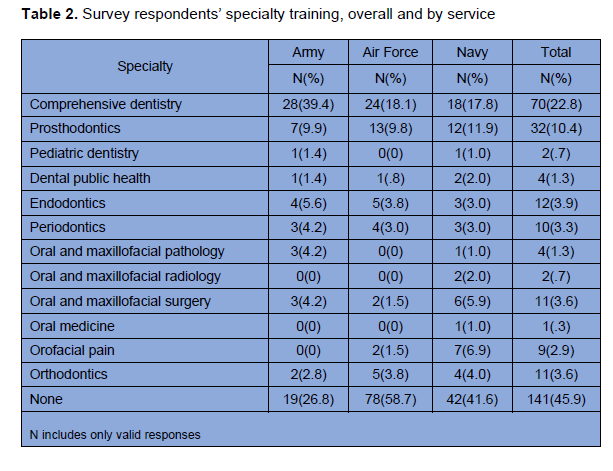
The vast majority (73.0%, n=243) of respondents reported completing a one-year advanced training program. Approximately half (54.1%, n=166) reported completing specialty training. Table 2 displays the specialty training of respondents by service. The specialty represented by the largest proportion (22.8%, n=70) was comprehensive dentistry followed by prosthodontics (10.4%, n=32).
Not all dentists who have had training in DSM are able to practice DSM in military dental clinics; specific military credentials and privileges are required to do so. Of the 190 dentists who reported they have received some type of DSM training, the vast majority (77.9%, n=148) noted they have the necessary credentials and privileges to practice DSM. Over one-third (38.2%, n=52) were comprehensive dentists, 15.4% (n=21) prosthodontists, and 6.6% (n=9) orofacial pain specialists.
Knowledge
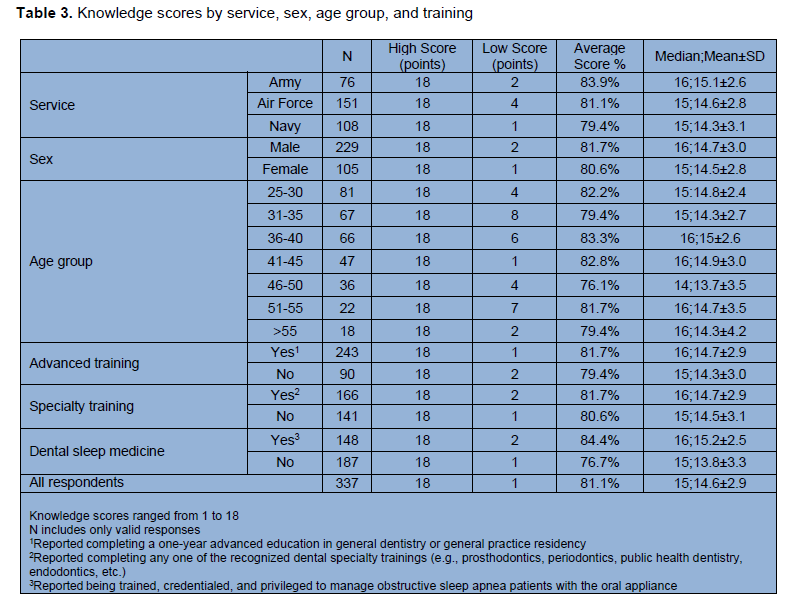
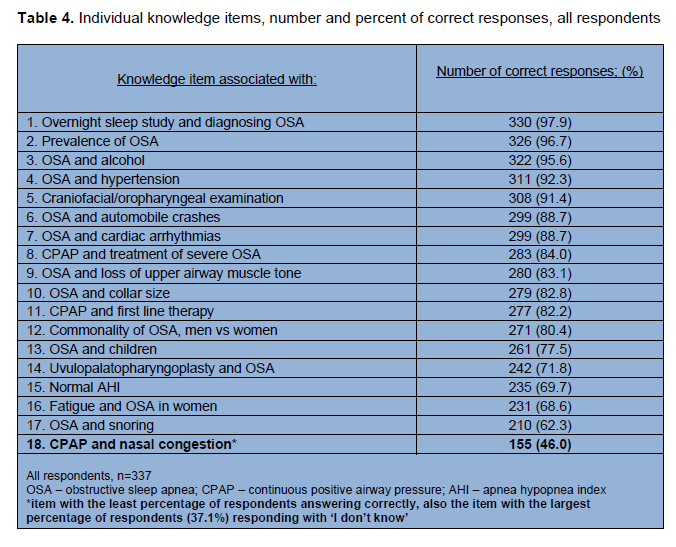
Table 3 displays OSAKA knowledge scores by service, sex, age group, and training. The lowest and highest knowledge scores for all respondents (n=337) were 1 and 18, respectively. The mean overall knowledge score was 14.6 (or 81.1%) and the median score was 15 (or 83%). When assessing knowledge scores by service, Army dentists had the highest mean score (15.1, or 83.9%) followed by the Air Force (14.6, or 81.1%) and finally the Navy (14.3, or 79.4%). Males had a slightly higher mean score (14.7, or 81.7%) compared to females (14.5, or 80.6%). Those who completed advanced training had a higher mean score (14.7, or 81.7%) compared to those who did not (14.3, or 79.4%). Specialty-trained dentists had a slightly higher mean score (14.7, or 81.7%) compared to non–specialty-trained dentists (14.5, or 80.6%). Those who reported practicing DSM had a higher mean score (15.2, or 84.4%) compared to those who did not practice DSM (13.8, or 76.7%). Dentists 36 to 40 years old had the highest mean score (15, or 83.3%) compared to all other age groups.Table 4 lists the number and percent of correct responses for each of the 18 individual knowledge items for all respondents. There was no single knowledge item that was answered correctly, or incorrectly, by all military dentists. The item with the greatest percent of dentists answering correctly (97.9%) was associated with diagnosing OSA using an overnight sleep study. The item answered correctly by the lowest percent of dentists (46.0%) inquired about the association of nasal congestion with PAP therapy. This item also had the greatest percent of dentists (37.1%) responding with “I don’t know.”
Attitudes
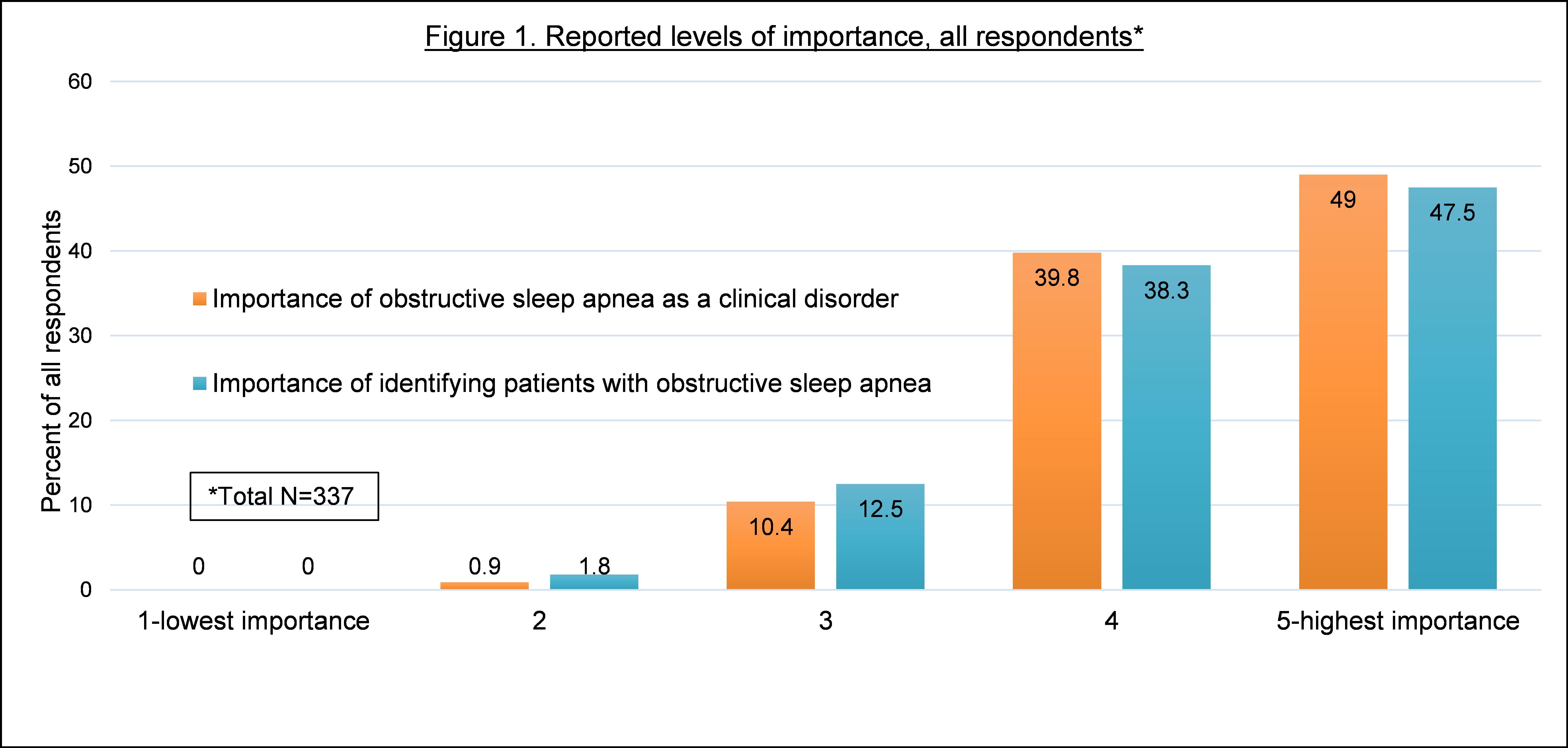
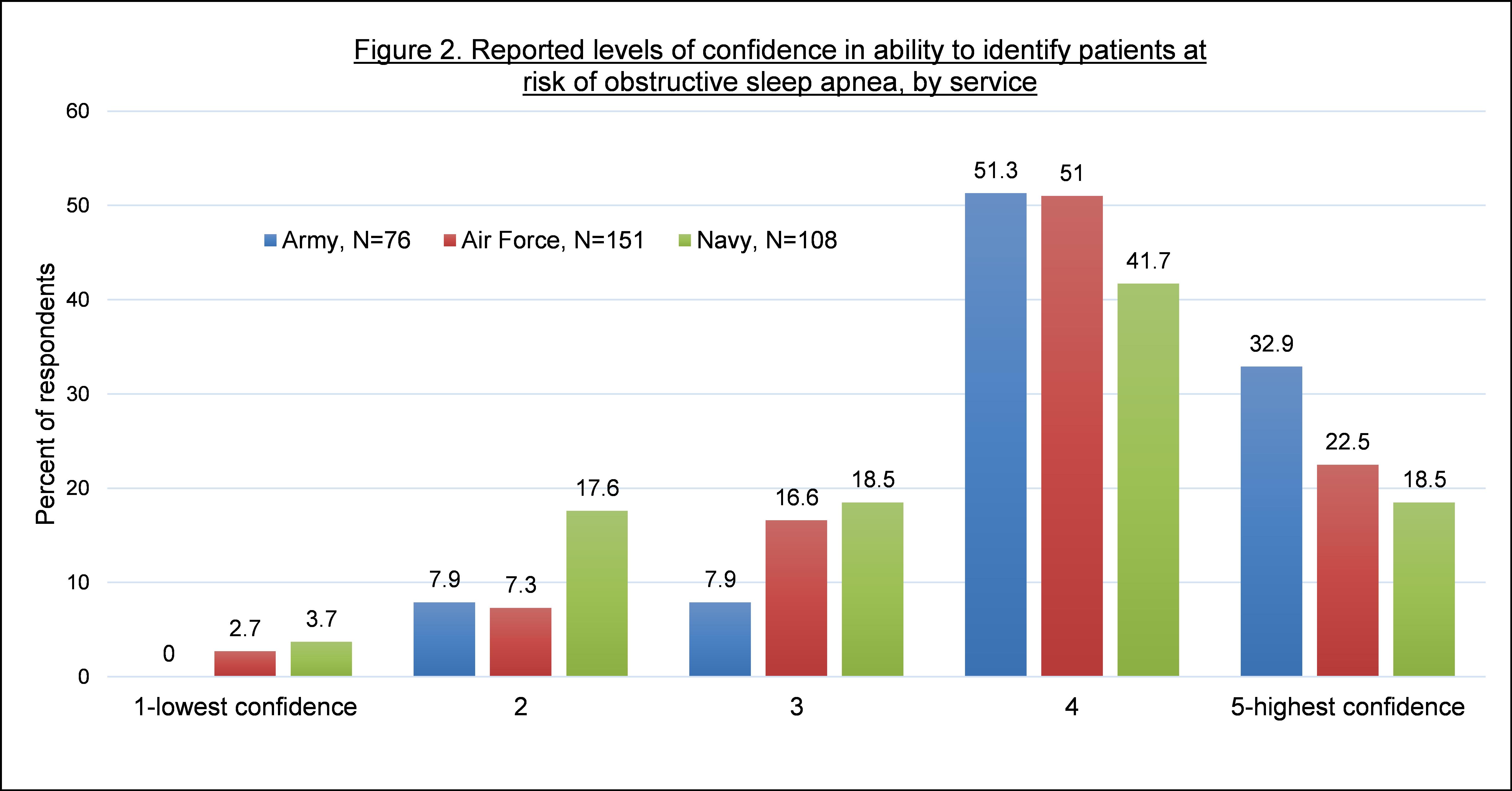
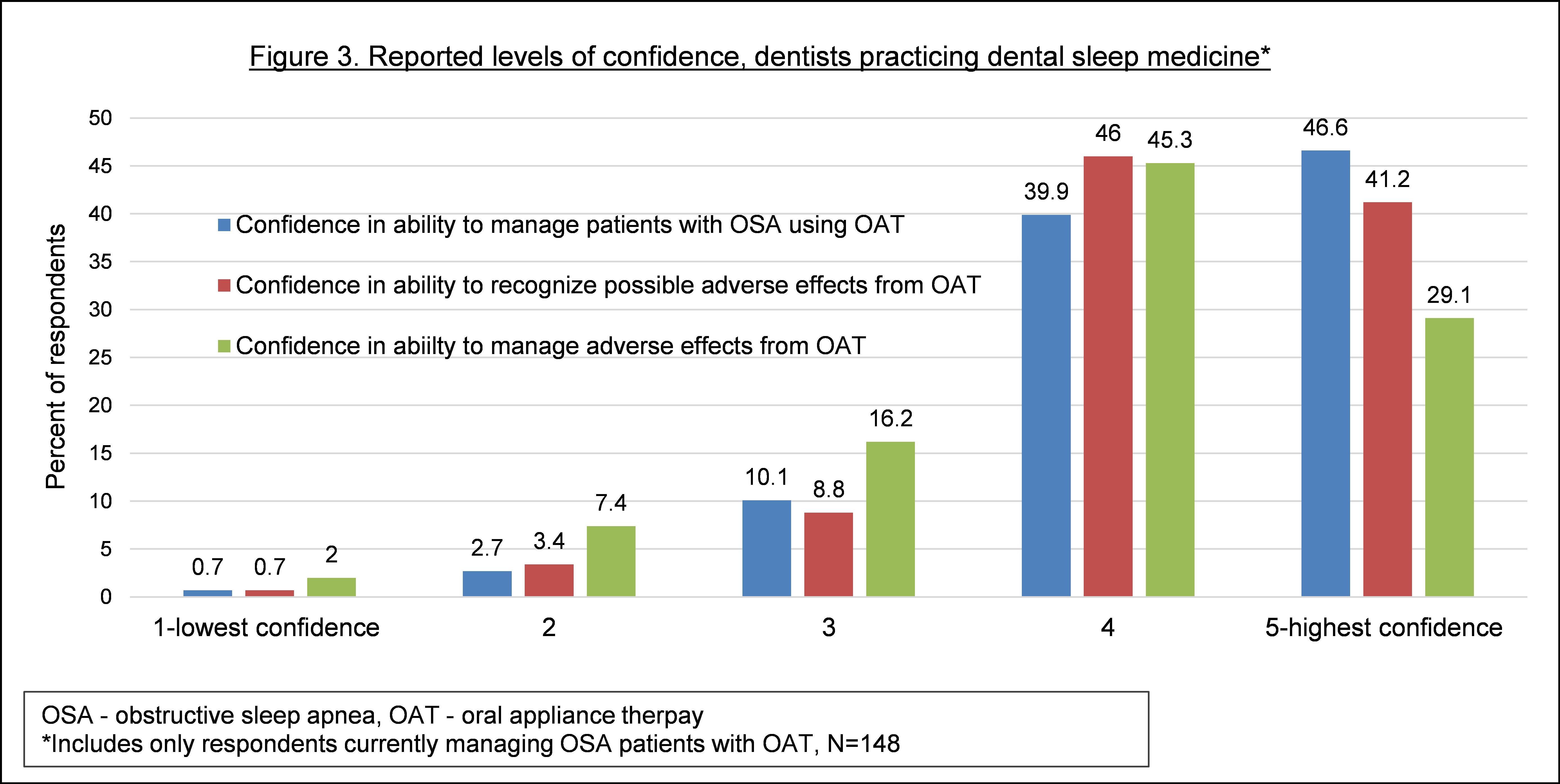
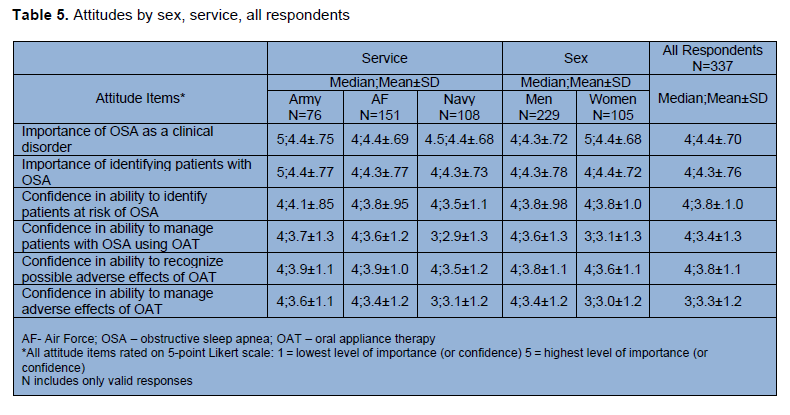
Following the OSAKA knowledge items, respondents were prompted with 6 separate attitude-related items asking them to rate the level of importance or confidence on a scale of 1 to 5; 1 represented the lowest level of importance (or confidence) and 5 represented the highest level of importance (or confidence). Figure 1 displays the frequency distributions of the first 2 attitude items for all respondents. The importance of OSA as a clinical disorder and the importance of identifying patients with it were both rated 5 by the greatest percent of dentists, 49% and 47.5%, respectively. Figure 2 displays the third attitude item, confidence in the ability to identify patients at risk of OSA, by service. The greatest percent of Army (51.3%), Air Force (51.0%), and Navy (41.7%) dentists rated their confidence level 4.Figure 3 displays the final 3 attitude (confidence) items. Only responses from DSM dentists (n=148) are shown in this figure. Confidence in the ability to manage patients with OSA using the oral appliance was rated 5 by the greatest percent (46.6%) of DSM dentists. Confidence levels in recognizing and managing adverse effects from the oral appliance were both rated 4 by the greatest percent of DSM dentists, 46% and 45.3%, respectively. Table 5 lists the medians and means of the 6 attitude items by sex, service, and overall. The 2 items with the lowest ratings included confidence in the ability to manage patients with OSA using the oral appliance (median = 3 for Navy and women) and manage adverse effects of the oral appliance (median = 3 for Navy, women, and for all respondents overall).
Table 1. Demographics of survey respondents |
{kind=link}
Table 2. Survey respondents’ specialty training, overall and by service |
{kind=link}
Table 3. Knowledge scores by service, sex, age group, and training |
{kind=link}
Table 4. Individual knowledge items, number and percent of correct responses, all respondents |
{kind=link}
Figure 1. Reported levels of importance, all respondents* |
{kind=link}
Figure 2. Reported levels of confidence in ability to identify patients at risk of obstructive sleep apnea, by service |
{kind=link}
Figure 3. Reported levels of confidence, dentists practicing dental sleep medicine* |
{kind=link}
Table 5. Attitudes by sex, service, all respondents |
{kind=link}
Associations Among Knowledge, Attitudes, and Age
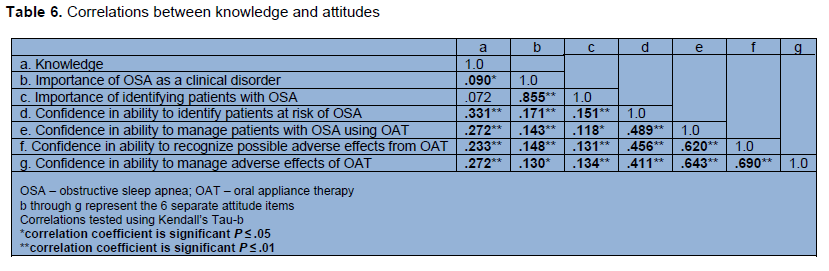
The strength and direction of association between each of the outcome variables are shown in Table 6. Knowledge was significantly, positively correlated with 5 of the 6 attitude items including the importance of OSA as a clinical disorder (P ≤ .05), confidence in the ability to identify patients at risk of OSA (P ≤ .01), manage patients with OSA using the oral appliance (P ≤ .01), recognize adverse effects from the oral appliance (P ≤ .01), and manage adverse effects from the appliance (P ≤ .01). All 6 individual attitude items were significantly, positively correlated with each other (P ≤ .05). The correlation between age and knowledge was not statistically significant; however, age was significantly, positively correlated with confidence in the ability to recognize (P = .007) and manage (P < .001) adverse effects from the oral appliance.Differences in Knowledge and Attitudes
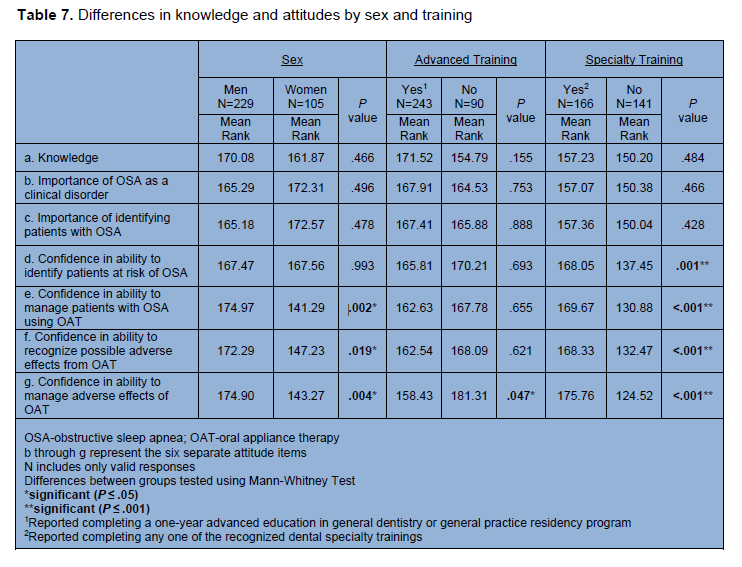
There were no statistically significant differences in knowledge scores by sex, one-year advanced training, or specialty training (Table 7). However, DSM dentists scored significantly higher compared to all remaining dentists (P < .001). Additionally, DSM dentists reported significantly higher confidence (all 4 confidence items) compared to all remaining dentists (P < .001). When compared to women, men reported significantly higher confidence in their ability to manage patients with OSA using the oral appliance (P = .002), recognize possible adverse effects from the oral appliance (P = .019), and manage adverse effects from the oral appliance (P = .004) (Table 7). Those who have not completed an advanced training program reported significantly higher confidence in their ability to manage adverse effects from the oral appliance (P = .047) compared to those who have completed advanced training. Compared to non–specialty-trained dentists, specialty-trained dentists reported significantly higher confidence (all four confidence items) (P ≤ .001).The Kruskal-Wallis H test indicated no statistically significant differences in knowledge between the three services. However, there were statistically significant differences in attitude (all 4 confidence items) between the services. Post hoc comparisons were made with an adjustment by the Bonferroni correction to determine where the differences lie between the three services. Reported confidence in the ability to identify patients at risk of OSA was significantly higher in the Army compared to the Navy (P ≤ .001). Reported confidence in the ability to manage patients with OSA using the oral appliance was significantly higher in the Army compared to the Navy (P =.000), as well as in the Air Force compared to the Navy (P =.000). Reported confidence in the ability to manage adverse effects from the oral appliance was significantly higher in the Army compared to the Navy (P =.015). Reported confidence in the ability to recognize possible adverse effects from the oral appliance differed significantly between the services (P = .038), though the post hoc test did not produce any significant pairwise comparisons.
Table 6. Correlations between knowledge and attitudes |
{kind=link}
Table 7. Differences in knowledge and attitudes by sex and training |
{kind=link}
DSM Practice Behaviors
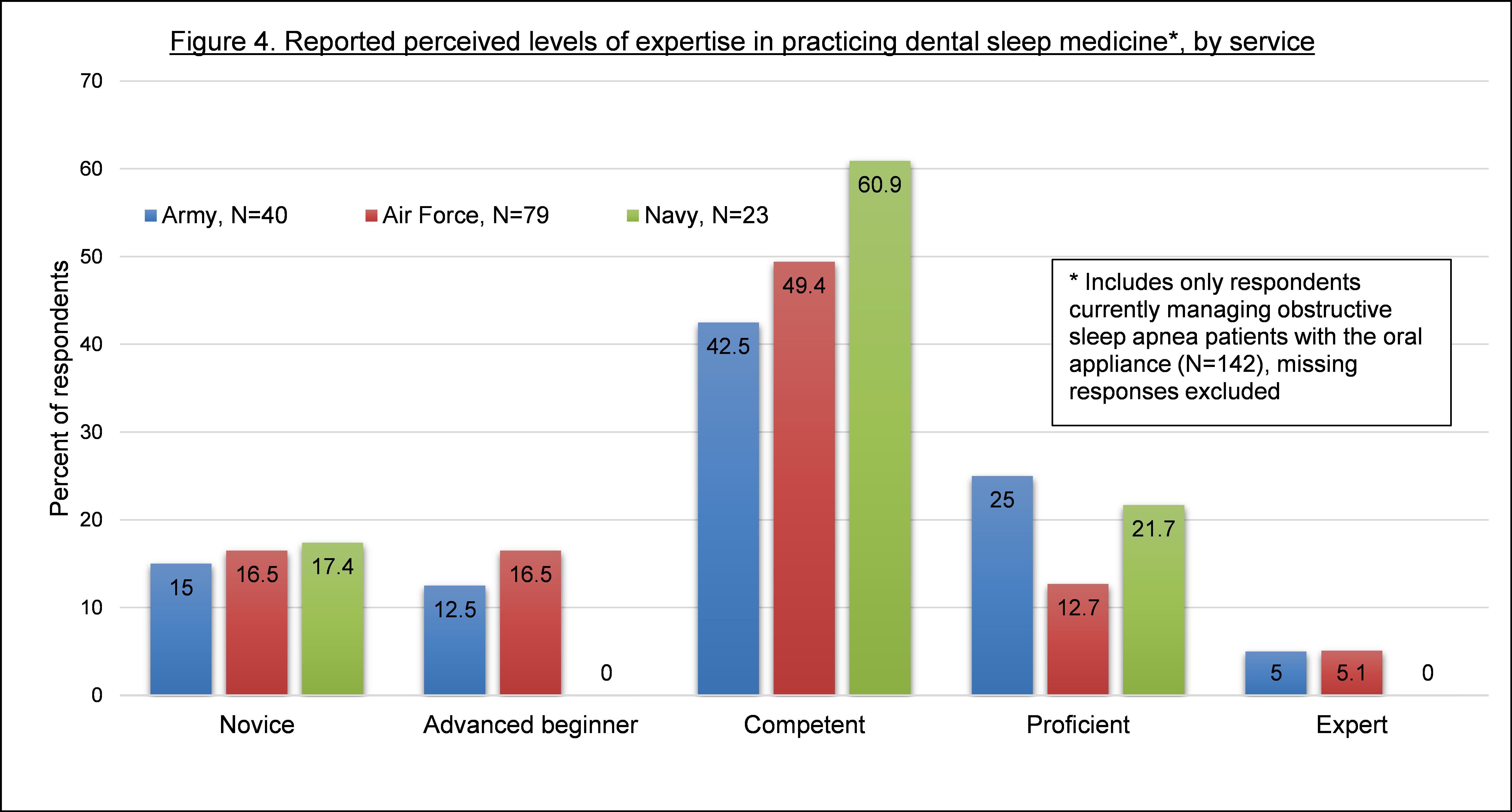
Following the completion of OSAKA, DSM dentists were asked additional questions regarding their practice behaviors including time in practice, perceived level of expertise, observed adverse effects from the oral appliance, management of those adverse effects, etc. The majority of dentists (68.5%, n=98) reported practicing DSM for 5 years or less; 35% (n=50) have practiced for 2 years or less. Respondents were asked to report the approximate number of appliances they deliver per month. The vast majority (79.7%, n=114) reported 2 appliances or fewer. Only 6 providers reported delivering 5 or more appliances per month.Options for perceived level of expertise in practicing DSM included novice, advanced beginner, competent, proficient, and expert. Most Navy (60.9%), Air Force (49.4%) and Army (42.5%) dentists rated themselves as competent (Figure 4). Only very small percentages of Army (5.0%) and Air Force (5.1%) dentists rated themselves as an expert. No Navy dentists selected expert. Of all DSM dentists who chose either proficient or expert (total n=31), almost half (48.4%, n=15) have been practicing DSM for 10 or more years; 45.2% (n=14) were comprehensive dentists, 32.3% (n=10) prosthodontists, and 9.7% (n=3) orofacial pain specialists.
Respondents were asked if they enjoy practicing DSM. The majority (57.3%, n=82) responded with “yes,” although, 30.8% (n=44) reported “sometimes.” Dentists had the opportunity to explain their answers by providing additional comments in a text box; 70 dentists provided remarks. For those who responded with “yes” some recurring comments included the following: oral appliance therapy can be life-changing for service members; it is a very rewarding treatment; it’s an incredible service to offer; it doesn’t just help patients, it helps their significant others; it provides patients with substantial benefits while requiring little chair time. Some who reported they do not (or only sometimes) enjoy practicing DSM attributed this to lack of collaboration between sleep medicine physicians and dentists, numerous adjustments the appliance requires, long lab fabrication turnaround time, adverse effects from the appliance, lack of confidence in providing the treatment because it is done so infrequently, and lack of confidence in the ability to manage adverse effects.
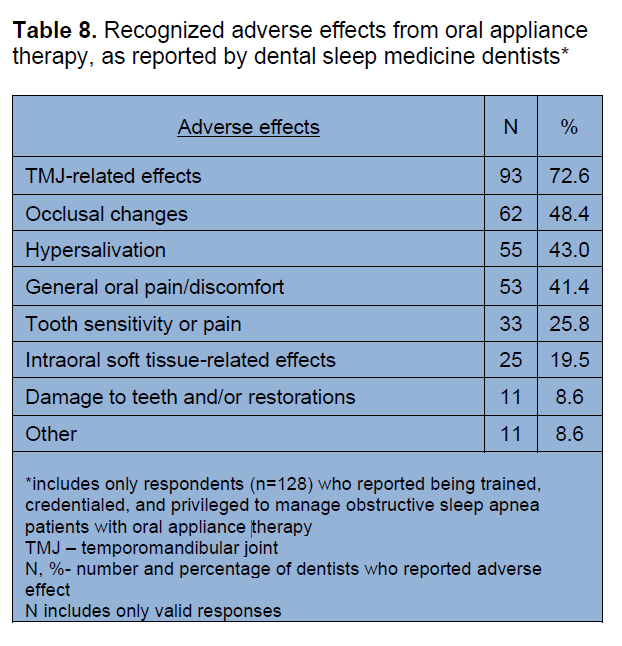
DSM dentists were presented with a list of possible adverse effects from the oral appliance and asked to select any they have ever witnessed while managing OSA patients. Table 8 lists these adverse effects as well as the number and percent of dentists who reported each. The most reported adverse effect, reported by 72.6% (n=93) of DSM dentists, was temporomandibular joint-related problems. This was followed by occlusal changes, hypersalivation, general oral pain/discomfort, tooth sensitivity/pain, intraoral soft-tissue effects, and damage to teeth and/or restorations. Eleven dentists (8.6%) reported “other” after which they were prompted with a text box to elaborate. Some responses included myalgia, xerostomia, claustrophobia, and removal of appliance by patient unknowingly during sleep. DSM dentists were asked if at any point the management of these adverse effects warranted referral to another dentist or dental specialist; 12.3% (n=17) of respondents reported “yes.”
DISCUSSION
While there are numerous studies that have administered surveys to evaluate the OSA-related knowledge among dentists, this is the first to employ the validated questionnaire, OSAKA, in assessing OSA knowledge and attitudes among tri-service military dentists (i.e., Army, Air Force, and Navy). Additionally, to the author’s knowledge, this is the first study to evaluate the DSM practice behaviors of tri-service military dentists trained in this subspecialty.
Table 8. Recognized adverse effects from oral appliance therapy, as reported by dental sleep medicine dentists* |
{kind=link}
Figure 4. Reported perceived levels of expertise in practicing dental sleep medicine*, by service
{kind=link}
A total of 337 Army, Air Force, and Navy dentists completed OSAKA with an overall mean knowledge score of 14.6 or 81.1%. The scores obtained in this study were not statistically compared with the OSAKA scores captured from any other studies. However, a descriptive, observational assessment between the results of this study and another follows below.
The mean knowledge score (81.1%) of military dentists was higher than that (73.6%) of the dentists surveyed with OSAKA in the 2021 study discussed earlier, a study that compared the knowledge scores of a sample of California dentists with those of various physician groups to determine if dentists were as knowledgeable about OSA as physicians.30 The group of physicians as a whole had a mean knowledge score of 63.9%. The physicians’ scores were also assessed by various specialty groups, including US and non-US groups. There were only 2 groups that had higher mean scores, albeit not much higher, than military dentists, including the Canadian otolaryngology residents (n=66, mean score 84.5%) and South African primary care physicians (n=41, mean score 83.6%).30 However, it is worth noting that the OSAKA survey used in the 2021 study was slightly different from the version distributed to military dentists. The 2021 study also evaluated the scores of each of the 18 individual knowledge items to determine where competencies (≥ 80% correct) and gaps (< 60% correct) existed.30 The California dentists exhibited 4 knowledge gaps (i.e., 4 of the 18 knowledge items were answered correctly by < 60% of respondents) and 9 competencies (i.e., 9 of the 18 items were answered correctly by ≥ 80% of respondents). The Canadian otolaryngology residents exhibited 15 knowledge competencies and 3 gaps.30,31 Using the same metric for this study, one might conclude this group of military dentists presented with 1 knowledge gap and 12 competencies (Table 4). The particular knowledge item answered correctly by less than 60% of military dentists was regarding PAP usage and nasal congestion, which was also one of the items the otolaryngology residents scored less than 60% on.30,31 An important point to consider regarding these knowledge scores is that while the assessment and management of patients with OSA are expected competencies for Canadian otolaryngology residents, they are not expected competencies for dentists.30,31
This study found no statistically significant differences in military dentists’ OSA knowledge scores by service, sex, age group, one-year advanced training, or specialty training. However, the groups with the highest mean knowledge scores in each of these categories included the Army, males, those in the 36-40 age group, those who completed advanced training (compared to those who did not), and those who are specialty-trained (compared to those who are not). Military dentists who reported they are DSM dentists, not surprisingly, scored significantly higher compared to that of all remaining military dentists. As mentioned previously, this study did not evaluate the differences in knowledge and attitude by each specialty and service due to the small sample sizes of those individual groups.
There was a significant positive correlation between age and confidence; as the age of military dentists increased so did their reported confidence in recognizing and managing adverse effects from the oral appliance. It can be expected that an increase in age would be accompanied by more experience and therefore, more confidence. One might also expect a higher knowledge score to accompany an increase in age, although that was not the case here as the correlation between knowledge and age was not statistically significant.
Discovering that DSM-practicing dentists reported significantly higher confidence (all 4 items) compared to all remaining dentists was expected. However, discovering that those who did not complete a one-year advanced training program reported significantly higher confidence (one item) compared to those who did complete an advanced training program was unexpected. One might assume that an additional year of training in general dentistry would lead to greater confidence; however, that was not the case here.
Overall, the more confident military dentists were in any one of the four confidence items, the more confident they were in the remaining items. Additionally, as their knowledge scores increased, so did their reported confidence (in all 4 items). Furthermore, the higher the military dentists’ knowledge scores, the more important they considered OSA as a clinical disorder.
When observing the frequency distribution of reported confidence levels among DSM dentists specifically (Figure 3), it was interesting to learn that most overall reported lower confidence levels in recognizing and managing adverse effects from the oral appliance compared to managing patients with OSA using the oral appliance. In this survey, DSM dentists had the opportunity to describe why they do or do not enjoy this particular area of general dentistry. A recurring comment from those who do not (or only sometimes) enjoy it described the multiple adverse effects they witnessed patients experiencing and their lack of confidence in being able to successfully manage them. An additional recurring comment included the lack of confidence in providing this treatment in general considering it is done so infrequently. The vast majority (79.7%) of DSM dentists reported delivering 2 or fewer oral appliances each month—a valuable point to consider when assessing their confidence and perceived levels of expertise. Most (49.7%) DSM dentists rated themselves competent in this field; very few (17.5%) selected proficient, and even fewer (4.2%) selected expert. Considering the additional comments provided as well as the reported confidence and perceived levels of expertise, it seems that the current DSM training process should include more time reviewing and discussing the possible adverse effects that may accompany oral appliance use as well as the appropriate methods of management. However, confidence and perceived expertise may improve on their own should military dentists begin providing this particular treatment more frequently than they currently do.
Limitations
Some limitations of this study include those inherent to using surveys and self-reported data, such as the introduction of unintentional biases and the inability to validate responses. While OSAKA is a validated survey, the remaining questions (i.e., the DSM practice behavior items) were not validated. However, those additional items only served as a method of collecting descriptive, subjective information regarding the practice of DSM in the military. Furthermore, OSAKA is not a test, meaning that the knowledge scores cannot be used to determine military dentists have a particular level of knowledge regarding OSA given that the scores are not validated against patient outcomes. Nevertheless, OSAKA scores can be used to compare different groups and/or as a needs-assessment.A distinct limitation of this study was the survey distribution method. Distribution was slow and inconsistent as it required the cooperation of numerous people from each service. However, it was the most expedient method available at the time. Additionally, a response rate cannot be calculated given that the number of dentists who received the survey is unknown. A final limitation includes the lack of generalizability as the number of respondents represents less than 12% of all military dentists.
CONCLUSIONS
OSA is a prevalent, deployment-limiting clinical disorder associated with considerable health complications as well as significant costs.1-13 Undiagnosed OSA is a health care concern warranting identification of service members at risk as early as possible to facilitate proper diagnosis and treatment. Untreated OSA can hinder a service member’s vigilance and performance, weaken a unit’s strength, and negatively impact mission success which, ultimately, may disrupt the efficiency and prowess of the military overall. Expanding the number of military providers screening for and treating OSA patients can help address this health care concern. Results of this survey suggest military dentists can and should be engaged in this effort. The majority of dentists who responded to OSAKA believe that OSA as a clinical disorder is greatly important, as is identifying those with it. Additionally, these dentists, overall, are confident in their ability to identify patients at risk of OSA. However, the results of this study are not representative of all military dental providers. Not all dentists are trained to recognize OSA risk factors or manage OSA patients with an oral appliance, as the amount of sleep-related education provided in dental school is minimal.
Further studies investigating the knowledge and attitudes of military dentists regarding OSA and oral appliance therapy are justified. Information gathered from these assessments will aid in developing OSA- and oral appliance therapy-related educational programs tailored specifically for military dentists. Broadening the roles of military dentists to include assisting in a multidisciplinary approach of OSA screening, diagnosis, and management will improve the health of service members, thereby advancing combat readiness, mission performance, mission success, and ultimately the military as a whole.
ACKNOWLEDGEMENTS
The author thanks Drs Helena M. Schotland and Donna B. Jeffe for providing permission to use the OSAKA questionnaire.29 Dr Jeffe is also thanked for her guidance and direction throughout the development and execution of this project. Likewise, Mr. Greg Markiewicz is much appreciated for his assistance with the fulfillment of the license agreement necessary to administer OSAKA.
REFERENCES
- Goodwin CE, Grier TL, Mahlmann OM. Obstructive sleep apnea surveillance and oral appliance therapy evaluation, active duty US army, 2014-2019. J Dent Sleep Med. 2024;11(1).
- Armed Forces Health Surveillance Center. Obstructive sleep apnea, active component, U.S. Armed Forces, January 2000–December 2009. MSMR. 2010;17(05):8–11.
- Rogers A, Stahlman S, Hunt D, Oh G, Clark L. Obstructive sleep apnea and associated attrition, active component, U.S. armed forces, January 2004-May 2016. MSMR. 2016; 23(10): 2-11.
- Moore B, Tison L, Palacios J, Peterson A, Mysliwiec V. Incidence of insomnia and obstructive sleep apnea in active duty United States military service members. SleepJ. 2021;44(7): zsab024.doi: 10.1093/sleep/zsab024.
- Haynes Z, Stewart I, Poltavskiy E, Holley, A, Janak, J, et al. Obstructive sleep apnea among survivors of combat-related traumatic injury: a retrospective cohort study. J Clin Sleep Med. 2022;18(1):171–179.
- Williams SG, Collen J, Wickwire E, Lettieri CJ, Mysliwiec V. The impact of sleep on soldier performance. Curr Psychiatry Rep. 2014;16(8):45.
- Health of the Force (2018). Defense Centers for Public Health – Aberdeen. https://phc.amedd.army.mil/Periodi-cal%20Library/2018HealthoftheForceReport.pdf
- Health of the Force (2019). Defense Centers for Public Health – Aberdeen https://phc.amedd.army.mil/PHC%20Re-source%20Library/2019_Health-of-the-Force.pdf
- Health of the Force (2020). Defense Centers for Public Health – Aberdeen https://phc.amedd.army.mil/PHC%20Resource%20Library/2020-hof-report.pdf
- Knowles S, Dekow M, Williamson M. Oral appliances for OSA treatment: meeting the quadruple aim. Military Medicine. 2023;188(3-4):e718-e724. https://doi.org/10.1093/milmed/usab316
- United States Central Command. USCENTCOM. Modification Seventeen (Tab A): Amplification of the Minimal Standards of Fitness for De-ployment to the CENTCOM AOR; to Accompany Modification Seventeen to USCENTCOM Individual Protection and Individual/Unit Deployment Policy. https://www.cent-com.mil/Portals/6/MEDICAL/MOD17_Tab_A.pdf
- Code of Federal Regulations, Title 30, Chapter 1, Part 4 – Schedule for rating disabilities. Authority 38 U.S.C. 1155. https://www.ecfr.gov/current/title-38/chapter-I/part-4#4.97
- U.S. Department of Veterans Affairs, Current disability compensation rates. https://www.va.gov/disability/compensation-rates/.
- Kryger M, Roth T, Goldstein C, Dement W. Principles and Practice of Sleep Medicine. 7th edition. Elsevier; 2022.
- Gottlieb DJ, Punjabi NM. Diagnosis and management of obstructive sleep apnea: a review. JAMA. 2020;323(14):1389-1400.
- Sateia MJ. International classification of sleep disorders-third edition: high-lights and modifications. Chest. 2014;146(5):1387-1394. doi:10.1378/chest.14-0970
- Walter Reed Army Institute of Research. Comprehensive fatigue manage-ment: maintaining cognitive dominance and the tactical advantage in multi-domain operations. https://me-dia.defense.gov/2023/Jul/26/2003268441/- 1/-1/1/COMPREHEN-SIVE-FATIGUE-MGMT-RELEVANCE-DOC-WRAIR-V1.PDF
- Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep.1997;20(9):705–706. doi: 10.1093/sleep/20.9.705.
- American Academy of Sleep Medicine, Obstructive Sleep Apnea Indicator Report. https://sleepeducation.org/wp-con-tent/uploads/2023/03/obstructive-sleep-apnea-indicator-report.pdf.
- Mantua J, Shevchik JD, Chaudhury S, Eldringhoff HP, Mickelson CA, McKeon AB. Sleep and infantry battle drill performance in special operations soldiers. Aerosp Med Hum Perform. 2022 Jul 1;93(7):557-561. doi: 10.3357/AMHP.6040.2022. PMID: 35859309.
- OTSG/MEDCOM Policy Memo 18-043, Dental Sleep Medicine Therapy (Obstructive Sleep Apnea and Severe Snoring Oral Appliance Ther-apy) in the U.S. Army Dental Care System, August 2018.
- Mysliwiec V, Capaldi V, Gill J,Baxter T, O’Reilly B, Matsangas P, Roth B. Adherence to positive airway pressure therapy in the U.S. military personnel with sleep apnea improves sleepiness, sleep quality, and depressive symptoms. Military Medicine. 2015;180(4):475-482.
- Lettieri CJ, Paolino N, Eliasson AH, Shah AA, Holley AB. Comparison of adjustable and fixed oral appliances for the treatment of obstructive sleep apnea. J Clin Sleep Med. 2011;7(5):439-445.
- Lim J, Lasserson T, Fleetham J, Wright J. Oral appliances for obstructive sleep apnea. Cochrane Database Syst Rev. 2006; 25(1):CD004435.
- American Dental Association (2019). Policy Statement on the Role of Dentistry in the Treatment of Sleep Related Breathing Disorders (Trans.2017:269;2019:270). https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/library/oral-health-topics/ada_2019_poli-cy_role_of_dentistry_sleep_related_breathing_disor-ders.pdf?rev=a6b7d4ff667c4325bd1cc402882e0235&hash=E95FE7655548C32764C7F5EE170A6A5A
- American Academy of Dental Sleep Medicine (2023). Scope of Practice. Approved by AADSM Board of Directors on 19 November 2023. https://www.aadsm.org/scope_of_practice.php
- Quan SF, Schmidt-Nowara W. The role of dentists in the diagnosis and treatment of obstructive sleep apnea: consensus and controversy. J Clin Sleep Med. 2017;13(10):1117-1119. doi:10.5664/jcsm.6748
- Gianoni-Capenakas S, Gomes AC, Mayoral P, Miguez M, Pliska B, Lagravere M. Sleep-disordered breathing: The dentists’ role – a sys-tematic review. J Dent Sleep Med. 2020;7(12020).
- Schotland HM, Jeffe DB. Development of the obstructive sleep apnea knowledge and attitudes (OSAKA) questionnaire. Sleep Med. 2003;4(5):443-450. [Erratum published Sleep Med. 2008;9:705.]
- Simmons M, Sayre J, Schotland H, Jeffe D. Obstructive sleep apnea knowledge among dentists and physicians. J Dent Sleep Med. 2021;8(4).
- Ansari S, Hu A. Knowledge and confidence in managing obstructive sleep apnea patients in Canadian otolaryngology - head and neck surgery residents: a cross sectional survey. J Otolaryngol Head Neck Surg. 2020;49(1):21. doi: 10.1186/s40463-020-00417-6
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted October 8, 2024
Submitted in final revised form January 21, 2025
Accepted for publication January 25, 2025
Address correspondence to: LTC Christa E. Goodwin, DMD, MS. Email: christa.goodwin@usuhs.edu