Original Article 1, Issue 12.1
An Assessment of Army Dentists’ Knowledge and Opinions of Obstructive Sleep Apnea
http://dx.doi.org/10.15331/jdsm.7366Jessica Bondy-Carey, DMD, MS, ABGD, Major, US Army Dental Corps
US Army AEGD-2 Hawaii
ABSTRACT
Objectives:
Obstructive sleep apnea (OSA) diagnoses continue to rise, particularly in military populations. However, current data suggest that OSA is still underdiagnosed. Dentists have the potential to play an important role in the management of OSA, especially in the military where Soldiers must receive annual dental examinations. The goal of this study was to establish and compare Army dentists with and without dental sleep medicine training and their current knowledge, comfort, and opinions regarding screening, patient referral, and their role in OSA management.
Methods:
An anonymous, voluntary survey link was emailed to 970 Army dentists. Questions included demographics, general knowledge of OSA, and Likert scale questions regarding the management of OSA.
Results:
A total of 223 dentists responded, comprising various experience levels (less than 1 year to more than 15 years practicing) and dental specialties. Approximately 25% of responders reported fewer than 5 hours of sleep medicine training. Untrained dentists were less knowledgeable of OSA, less likely to screen patients for OSA, and were more likely to report being uncomfortable with screening or referral to a physician for evaluation of suspected OSA. All groups agreed dentists play a role in OSA management, and that increased sleep medicine training would benefit their practice.
Conclusion:
The results indicate sleep medicine training increases Army dentists’ knowledge and comfort in screening, patient referral, and management of OSA.
Clinical Implications:
Increasing the number of dentists trained and comfortable managing OSA would increase identification, diagnosis, and access to care for management of OSA.
Keywords:
Obstructive sleep apnea, OSA, military, Army, opinion, screen, train, refer
Citation:
Bondy-Carey J. An assessment of army dentists’ knowledge and opinions of obstructive sleep apnea. J Dent Sleep Med. 2025;12(1)
INTRODUCTION
Obstructive sleep apnea (OSA) diagnoses continue to rise in the United States. The prevalence of OSA in the United States is estimated between 22 to 28 million adults; the diagnosis is made in only approximately 6 million patients.1 Despite the serious sequelae of untreated OSA, studies indicate effective screening and identification remain low, with approximately 80% to 90% of OSA cases undiagnosed.2 Despite being a relatively healthy population, service members are also at risk, with studies indicating a marked increase in OSA diagnoses among military service members since 2005.3,4
Military service members are often expected to remain attentive in hazardous environments and situations. Concentration is required during training and combat operations as service members are often operating heavy machinery, vehicles, and weapons that can affect the safety of many people. Therefore, the Army has long recognized the importance of quality, timely sleep and promotes optimizing health with a performance triad that includes sleep. OSA, however, negatively affects patients as well as those around them. Countless studies have demonstrated the deleterious effects snoring in patients with OSA on the sleep quality of bed partners.5 The applicability of this concept is particularly true for service members because during training and deployment they are often in very close sleeping quarters with one another. If service members are struggling with undiagnosed or untreated OSA, the sleep quality and potential adverse effects could disrupt entire units of soldiers. The compounding consequence of OSA could potentially decrease unit morale, cohesion, and effectiveness.
OSA may be characterized by intraoral signs and symptoms that can be noticed or reported by the patient during routine dental appointments. Possible intraoral signs include enlarged or scalloped tongue, mandibular tori, periodontitis, retrusive jaw, redness of the soft palate, and narrow palate.6-10 These signs may also be accompanied by symptoms including temporomandibular dysfunction, dry mouth, bruxism, depression, daytime sleepiness, fatigue, and snoring.6-10 Although these signs and symptoms are by no means exclusive to OSA and are still debated among dental and medical sleep experts, patients presenting with several of these signs or symptoms should alert the dental professional to screen and refer as needed for possible OSA.
Previous studies have sought to establish how dentists fit into the OSA conundrum. The first published article regarding dentists’ knowledge and perceptions of OSA was in 2004 by Bian.11 In this study, 58% of surveyed dentists could not identify common intraoral and reported signs and symptoms of OSA, and there was limited communication between dentists and physicians.11 Approximately 15 years later, a group of researchers from Riyadh used a questionnaire-based study to once again demonstrate a significant lack of OSA knowledge among graduating dental students.12 However, Kale et al. assessed the knowledge and attitude about various areas of OSA of dentists at a dental college in India. They found that although dentists had a good general knowledge of OSA, they had poor familiarity with screening, diagnosis, patient referral, and treatment of patients with OSA.13 In yet another study, a group from Helsinki (Vuorjoki-Ranta et al.) compared general dentists and specialists and their knowledge and attitudes about OSA. They found specialists had more knowledge of OSA and recommended increased OSA education in dental school and better cooperation among medical professionals and development of adherent treatment chains.14 Finally, a survey sent to a limited group of Army dentists at Fort Bragg in 2019 by Balkom and Beltran concluded that dental specialty, sex of the dental specialist, and history of OSA training did not have significant effect on OSA knowledge, but approximately 50% of Army dentists did not feel confident in their OSA training.15
Researchers around the world have dedicated time and resources in attempts to understand the potential ramifications of OSA. It is estimated that approximately 1 billion people around the world have OSA.16 In the United States, a report from the market research company Frost & Sullivan (as commissioned by the American Academy of Sleep Medicine) estimated that undiagnosed OSA cost the United States approximately $149.6 billion in 2015.1 A study published by the United States Navy conveyed that the 1 in 20 service members with sleep-disordered breathing cost taxpayers approximately $100 million in fiscal year 2012 to 2013 and this cost would continue to rise.5 The rising costs of treating the adverse health consequences of patients with OSA will overburden healthcare system resources and personnel.1,4,5 Medical organizations globally will need to consider innovative, cost-effective, and practical approaches to managing OSA.
As OSA continues to burden the medical system, dentists have the potential to play an important role in solving the screening, referral, and treatment of patients with OSA. Several position papers have been published highlighting the need for a multidisciplinary approach to OSA management and dentists’ role on that team.17-20 In 2017, the American Dental Association policy “The Role of Dentistry in the Treatment of Sleep Related Breathing Disorders” emphasized that dentists should be screening patients for sleep-related breathing disorders as part of their comprehensive examinations and if a risk of sleep-related breathing disorder is suspected, patients should be referred for evaluation and diagnosis by a physician.17 Despite published American Dental Association (ADA) guidelines regarding dentists and sleep-related breathing disorder, it appears many private practice and military dentists are not conducting routine OSA screenings at yearly dental examinations.2,15 It is unclear, though, whether this is because dentists are not adequately educated and trained in sleep medicine, or if they do not think it is within their scope of practice to screen, refer, and manage patients with OSA. Still, there are limited studies offering comprehensive analysis of dentists’ management of OSA and, to the authors’ knowledge, there is no study comparing the effect of sleep medicine training on Army dentists’ knowledge and opinions regarding screening, referral, and OSA therapy and the potential implications this has on OSA identification, treatment, and Soldier readiness.
The United States Army Dental Corps offers an excellent opportunity to study this topic because it includes a cohort of dentists trained from dental schools across the United States, a variety of experience levels and specialists, and provides the opportunity for some Army dentists to take a sleep medicine course. Additionally, Army dentists are treating an at-risk population who are required to receive an annual dental examination and have access to free medical and dental care.
OBJECTIVE
It is the authors’ goal to establish Army dentists’ current knowledge regarding signs and symptoms, screening methods, and OSA therapy. Additionally, this study sought to determine Army dentists’ comfort level with screening and referring OSA as well as their opinions of dentists’ role in OSA management. Finally, the author wanted to compare the effect of sleep medicine training on Army dentists’ knowledge and opinions of OSA. It is hypothesized that Army dentists without dental sleep medicine training have limited knowledge of OSA and are less confident in screening methods and referring possible patients with OSA.
METHODS
A survey was developed for this research project and a link to a voluntary, web-based survey was emailed through Outlook to a distribution list containing all active-duty Army dentists (970 total recipients). The email explained the purpose of the survey, how long it would take to complete, that no personal identifiable information would be collected, and that by clicking the link they consented to participate in the survey but could withdraw consent at any point by exiting the browser.
Questions included demographics and training, knowledge-based questions regarding definitions, signs, symptoms, and screening for OSA, and Likert scale questions concerning comfort for screening, referral, and dentists’ role in OSA identification and treatment. A final option to leave any additional comments or opinions about the survey or dental sleep medicine was afforded to survey participants. The survey remained opened for 2 months before it was closed, and a statistical analysis was performed.
Statistical Analysis
Kruskal-Wallis tests were performed to assess group differences with respect to training and beliefs regarding OSA. Pearson chi-square tests were used to assess pairwise differences where appropriate. Pooling of respondent data was conducted to facilitate group comparisons. Consequently, those responding ‘Yes’ and reporting more than 5 hours of OSA and/or dental sleep medicine training were grouped together as trained (n= 165) and those responding ‘No’ or reporting fewer than 5 hours of training were grouped together as untrained (n= 68). Because the goal of this research was to establish Army dentists’ knowledge and opinions of OSA and the potential effect of any OSA training on that, 5 hours was chosen because it likely indicates the dentist has had more than a brief overview or introduction to OSA. It does not indicate they are certified or qualified in dental sleep medicine, merely that they have likely received additional training through residency, or a course dedicated specifically to sleep medicine. Data were analyzed using Statistical Package for the Social Sciences version 25 (IBM, Armonk, NY, USA). Statistical significance for all statistical tests was declared at P < 0.05.
RESULTS
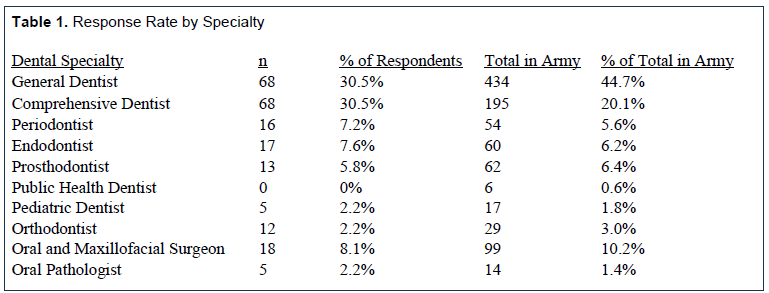
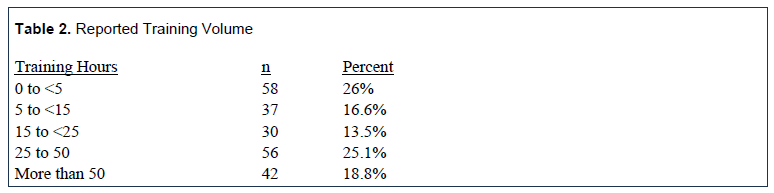
Among the 970 dental specialists contacted regarding the survey, 22.9% (n = 223) completed the survey. Respondents included the following: general dentists (n = 68, 30.5%); comprehensive dentists[1] (n = 68, 30.5%); oral and maxillofacial surgeons (n = 18, 8.1%); endodontists (n = 17, 7.6%); periodontists (n = 16, 7.2%); prosthodontists (n =13, 5.8%); orthodontists (n = 12, 5.4%); oral pathologists (n = 5, 2.2%); and pediatric dentists (n = 5, 2.2%). Table 1 shows the percentage of respondents by specialty as well as the total number of each specialty in the Army. General dentists reported less experience overall in comparison with the other dental specialties, P<0.001. When asked about OSA training, 26% of participants reported zero to fewer than 5 hours of sleep medicine or OSA training. General dentists with no residency training were the most likely to report fewer than 5 hours of dental sleep medicine training. The amount of training received is outlined in Table 2. Most trained respondents reported having OSA training during a residency program (63.7%), followed by the Army dental sleep medicine course (41.7%), dental school (25.1%), continuing education courses (10%), and the American Academy of Dental Sleep Medicine (9.9%).
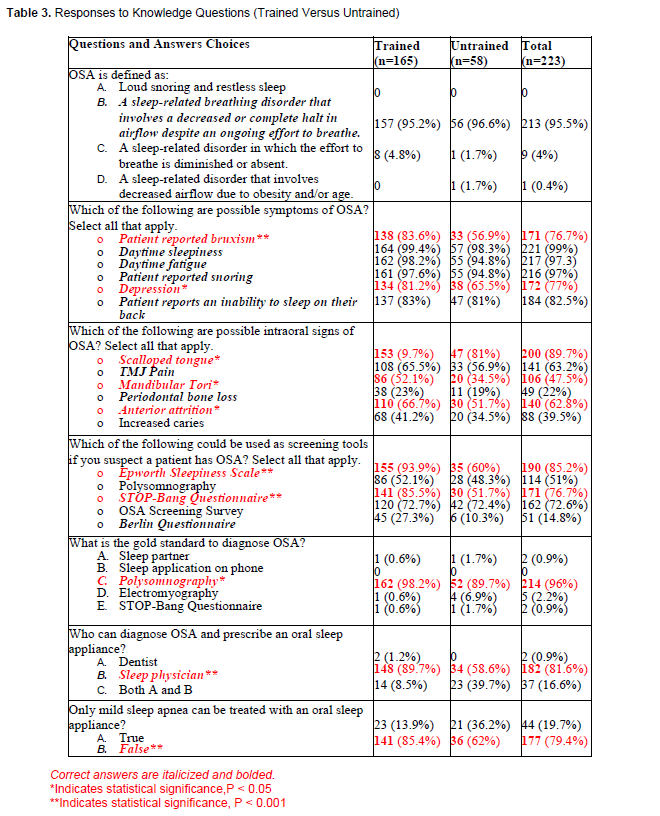
Then respondents were asked questions to test their knowledge of OSA. Although most respondents answered questions about OSA diagnosis and screening correctly, trained dentists were significantly more likely to respond correctly (P<0.05). Additionally, 72.6% and 50.6% incorrectly chose the OSA screening survey (a vague description and not a specific test) and polysomnography (respectively) as screening tools, whereas few dentists (14.8%) were familiar with the Berlin Questionnaire. When asked to identify possible symptoms of OSA, almost all respondents correctly selected daytime sleepiness (99.1%), snoring (96.9%), daytime fatigue (97.3%) and inability to sleep on one’s back (82.1%). However, more subtle symptoms including nocturnal bruxism (76.7%) and depression (77.1%) were more likely to be selected by trained dentists (P<0.05). Trained dentists were significantly more likely to select scalloped tongue, mandibular tori, and anterior attrition (P<0.05) as intraoral signs of OSA than their untrained counterparts. Approximately 40% of Army dentists incorrectly selected increased caries. Specific questions are displayed in Table 3 as well as comparisons between trained and untrained dentists.
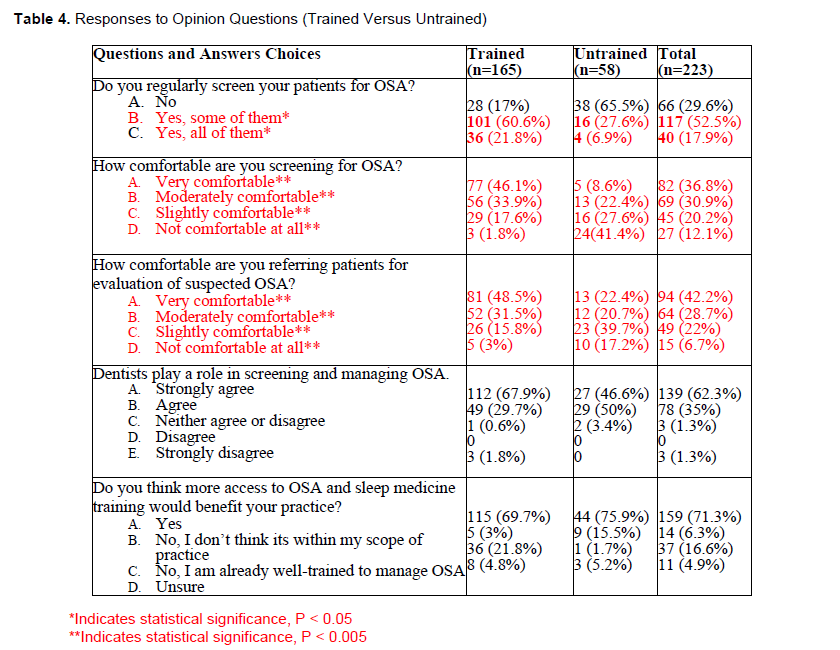
Next, participants answered Likert scale opinion-based questions regarding OSA management. Approximately one-third of Army dentists reported not being comfortable or only slightly comfortable screening and referring for evaluation of suspected OSA. Moreover, 29.6% of Army dentists indicated they did not screen any of their patients. Additionally, individuals with OSA training were significantly more comfortable screening and referring for suspected OSA, P<0.001. Finally, when asked if dentists play a role in diagnosing and providing treatment for OSA, most respondents (97.3%) indicated they do. Seventy-one percent of respondents indicated they would benefit from additional training while the remaining participants had deferring opinions.
Complete questions with trained versus untrained comparisons are presented in Table 4.
Table 1. Response Rate by Specialty |
{kind=link}
Table 2. Reported Training Volume |
{kind=link}
Table 3. Responses to Knowledge Questions (Trained Versus Untrained) |
{kind=link}
Table 4. Responses to Opinion Questions (Trained Versus Untrained) |
{kind=link}
DISCUSSION
The results of this study support the hypothesis that Army dentists without dental sleep medicine training have statistically significantly less knowledge of OSA and are less confident in screening and referring possible patients with OSA in comparison with their trained counterparts.
Furthermore, this study establishes Army dentists’ current knowledge about OSA as well as their attitude toward screening, referral, and management of patients with OSA. Finally, it also offered an assessment of the effect of sleep medicine training on Army dentists’ knowledge and opinions of OSA.
A strength of this study was the number of responses and the diverse experience level and dental specialty demographics of the group. Dental practice experience ranged from less than 1 year to more than 15 years and dentists from a variety of specialties.
Another unique feature of this survey was its specific examination of whether dentists had received any training about OSA or sleep medicine, where they had received it, and how much training they had. Of those trained, most reported their training was during residency or the Army sleep medicine course. Surprisingly, only 25% of Army dentists reported OSA training during dental school. Additionally, general dentists with no residency training were the most likely to report fewer than 5 hours of dental sleep medicine training. Therefore, if general dentists are not being trained in dental school, in residency, or the Army sleep medicine course, they are likely not properly trained to identify and screen for OSA during dental examinations. This was evident in the survey, as untrained dentists were less likely to identify intraoral signs of OSA. This is particularly problematic for the Army because general dentists perform most patient screenings and examinations. Additionally, they see the most patients and serve as the conduit for treatment elevation within the dental system. If they are not proficient in identifying and screening patients for OSA, there is a high likelihood OSA is undiagnosed in many potential patients.
Overall, this study demonstrated Army dentists had a good baseline knowledge of OSA. Most Army dentists could correctly define OSA, understood it had to be diagnosed via polysomnography and a physician, and could identify well-known symptoms of OSA. However, the more subtle symptoms, though, such as patient-reported bruxism and depression were statistically more likely to be identified by trained dentists. Therefore, the potential sequalae of bruxism, including temporomandibular disorder, myofascial pain, headaches, and tooth damage, are less likely to be attributed to OSA by untrained dentists. This could prove frustrating to both providers and patients as chief complaints and sick call visits are never truly solved because the correlation between OSA and these symptoms is never made.
Without question, dentists should be able to routinely identify signs and symptoms of OSA and subsequently screen and refer for suspected OSA evaluation. Even though 97% of respondents agreed that dentists play a role in screening and treating patients with OSA, only 18% screen all patients for OSA. More worrisome is that approximately 30% of Army dentists are not regularly screening their patients for OSA. Careful consideration of several of the survey questions may offer valuable insight as to other reasons why this number remains so high. First, most dentists receive no OSA or sleep medicine training during dental school. Therefore, if postgraduate training is not provided, there is a high probability that dentists lack proper skills to screen and treat patients with OSA. It is also possible that dentists do not realize it is not only within their scope of practice to screen, refer, and treat patients with OSA, but that there is an ADA policy recommending dentists provide regular OSA screenings during dental examinations. Likewise, there is no official military policy or regulation requiring or standardizing OSA screenings as part of dental or medical yearly examinations. Despite ADA recommendations, there likely are more regulations restricting Army dentists from treating patients with OSA, such as local command policies and credentialing committee limitations placed on privileges.
Second, one of the more enlightening and different aspects of the survey was the effect of training on dentists’ reported comfort about OSA management. Trained providers were significantly more comfortable screening and referring for suspected OSA. There was a significant correlation between those who reported screening for OSA and those who reported being comfortable screening for OSA. Consequently, lack of confidence in their training or not knowing how to apply their knowledge in a clinical setting to confidently screen and refer patients may also explain why some dentists are not screening patients for OSA.
Third, the final question of the survey allowed space for any comments or questions about the survey or sleep medicine. Like previous studies,11,14 several commented that their biggest difficulty was communicating with physicians. Conversely, medical providers may not be aware that Army dentists provide oral appliance therapy, thereby underutilizing Army dentists. This is a huge disservice to patients and can lead to delayed care, denied insurance claims, and patient dissatisfaction. Without clear, established communication chains, it can become cumbersome, impractical, and discouraging for dentists to refer patients with suspected OSA for evaluation.
Finally, several Army dentists also reported they did not think that they had the support of their commanding officer. Some stated their commanding officer did not readily provide sleep medicine course training information and did not support training opportunities for their dentists, especially the general dentists. Others reported commanding officers denying credentialing to trained providers. This presents an interesting military perspective as Army dentists are not only subject to state licensure laws and ADA guidelines, but also local military policies, adding an additional barrier for dentists to navigate. It is hoped that by demonstrating the significant effect of sleep medicine training on Army dentists’ knowledge and confidence in the treatment of patients with OSA that it will help promote awareness to Army dental leadership to the importance of properly training Army dentists about OSA, increase training opportunities (especially for general dentists), and create policies to incorporate regular OSA screenings into yearly military dental exams.
A limitation of this study is that the statistics are based on a specific cohort (Army dentists) in a unique environment. Although many of the conclusions drawn from this study could be applied to civilian dentists, undoubtedly they have many factors that would uniquely affect their practices and responses. These include insurance, finances, communication with physicians, and production. Additionally, it is important to note that specialists make up 55% of Army dentists while they only comprise 20% of civilian dentists. This is likely why 75% of Army dentists reported more than 5 hours of OSA training and perhaps why (in comparison with the aforementioned studies) Army dentists receive more dental sleep medicine training than civilian dentists. Therefore, the results of this study may overinflate the general knowledge and comfort of dentists in treating patients with OSA. Additional studies are needed to completely understand the dynamic role dentists play in OSA management.
CONCLUSIONS AND RECOMMENDATIONS
The results of this study indicate that in comparison with their trained counterparts, Army dentists without sleep medicine training were statistically less knowledgeable and confident with screening and referral of patients suspected of having OSA . This suggests increased sleep medicine training would increase Army dentists’ knowledge and confidence in screening and referral of patients with OSA. Furthermore, local commanding officer support for increased sleep medicine training and credentialling and improving communication with physicians would empower more Army dentists to screen and treat patients with OSA. Army dentistry has the potential to make a significant effect on the rising health concern surrounding OSA. By training more providers and implementing routine OSA screenings into yearly dental examinations, access to care, screening, referral, and diagnosis of OSA would increase. Ultimately, this would improve readiness and deployability of soldiers.
ACKNOWLEDGEMENT
The author would like to express gratitude to Mr. Thomas Beltran for his statistical analysis, as well as program directors Dr. Charles Lambert and Dr. Nick Wilson.
DISCLAIMER
The views expressed in this article are those of the author and do not reflect the official policy or position of the US Army Medical Department, Department of the Army, Department of Defense, or the US Government.
REFERENCES
- Hidden Health Crisis Costing America Billions: Underdiagnosing and Undertreating Obstructive Sleep Apnea Draining Health Care System. American Academy of Sleep Medicine. https://aasm.org/resources/pdf/sleep- apnea-economic- crisis.pdf. August 2016; Accessed May 7, 2023.
- Chiang H, Long A, Carrico C, Rodinson R. The prevalence of general dentists who screen for obstructive sleep apnea. J Dent Sleep Med. 2018;5(3):55-60.
- Moore BA, Tison LM, Palacios JG, Peterson AL, Mysliwiec V. Incidence of insomnia and obstructive sleep apnea in active-duty United States military service members. Sleep. 2021; 44(7).
- Eliason M, Jardine D, Pelchy K, Meyer C, McIntyre N. Sleep-disordered breathing in the active-duty military population and its civilian care cost. Federal Practitioner. 2017;34(2):32-36.
- Beninati W, Harris CD, Herold DL, Shepard JW Jr. The effect of snoring and obstructive sleep apnea on the sleep quality of bed partners. Mayo Clin Proc. 1999;74(10):955-8.
- Berggren K, Broström A, Firestone A, Wright B, Josefsson E, Lindmark U. Oral health problems linked to obstructive sleep apnea are not always recognized within dental care-As described by dental professionals. Clin Exp Dent Res. 2022; 8(1):84-95.
- Billings ME. Putting some teeth into it: Connecting periodontitis with sleep apnea. Sleep. 2015;38(8):1153-4.
- Weiss TM, Atanasov S, Calhoun KH. The association of tongue scalloping with obstructive sleep apnea and related sleep pathology. Otolaryngol Head Neck Surg. 2005;133(6):966-71.
- Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA cohort. J Dent Res. 2013;92(7 Suppl):70S-7S.
- Jehan S, Auguste E, Pandi-Perumal SR, et al. Depression, obstructive sleep apnea and psychosocial health. Sleep Med Disord. 2017;1(3):00012.
- Bian H. Knowledge, opinions, and clinical experience of general practice dentists toward obstructive sleep apnea and oral appliances. Sleep Breath. 2004;8(2):85-90.
- Swapna LA, Alotaibi NF, Falatah SA, Joaithen M, Koppolu P. Knowledge of obstructive sleep apnea among dental fraternity in Riyadh. Open Access Maced J Med Sci. 2019;7(15):2508–12.
- Kale SS, Kakodkar P, Shetiya SH. Obstructive sleep apnea domains: knowledge, attitude and practice results of dentists from a dental college in India. Sleep Sci. 2020;13(1):3- 9.
- Vuorjoki-Ranta TR, Lobbezoo F, Vehkalahti M, Tuomilehto H, Ahlberg J. Treatment of obstructive sleep apnea patients in community dental care: knowledge and attitudes among general dental practitioners and specialist dentists. J Oral Rehabil. 2016;43(12):937-942.
- Balkom GA, Beltran T. An evaluation of the opinions and knowledge on obstructive sleep apnea at the Fort Bragg DENTAC. USU Theses, Dissertations, and DNP Projects. https://digitalcollections.lrc.usuhs.edu/digital/collection/p16005coll10/id/146221/rec/6. May 2019; Accessed September 2021.
- Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698.
- The Role of Dentistry in the Treatment of Sleep Related Breathing Disorders. American Dental Association website. https://www.ada.org/-/media/project/ada-organization/ada/ada-org/files/resources/research/the- role-of-dentistry-in-sleep-related-breathing-disorders.pdf. Published 2019; Updated January 2023; Accessed May 15, 2023.
- Gauthier L, Almeida F, Arcache JP, et al. Position paper by Canadian dental sleep medicine professionals on the role of different health care professionals in managing obstructive sleep apnea and snoring with oral appliances. Can Respir J. 2012;19(5):307-9.
- Schwarting S, Huebers U, Heise M, Schlieper J, Hauschild A. Position paper on the use of mandibular advancement devices in adults with sleep-related breathing disorders. A position paper of the German Society of Dental Sleep Medicine (Deutsche Gesellschaft Zahnaerztliche Schlafmedizin, DGZS). Sleep Breath. 2007;11(2):125-6.
- Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep. 2006;29(2):240-3.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted September 6, 2023
Submitted in final revised form January 18, 2024
Accepted for publication August 14, 2024
Address correspondence to: Jessica Bondy-Carey, DMD, MS, MS. Address: 10205 S. Riva Ridge Loop, Fort Drum, NY 13602. Email: JLBond02@gmail.com