Original Article 1, Issue 11.2
Daylight Saving Time and Self-Reported Bruxism Manifestations: First Results From a Multicentric, Case-Control Study
http://dx.doi.org/10.15331/jdsm.7328Miguel Meira e Cruz, DDS, MSc,1, Izabella Paola Manetta, DDS,2, David Gozal, MD, PhD,3, Antonio Romero-Garcia, DDS, PhD,4, Pedro Cebola, DDS,5, Jose Torres- Hortelano, DDS, PhD,6, Maria Victoria López Molla, DDS, PhD,7, Dominik Ettlin, DDS, PhD8
1 Sleep Unit, Centro Cardiovascular da Universidade de Lisboa, Lisbon School of Medicine, Lisbon, Portugal, 2 Pontificia Universidade Catolica de Campinas, Otolaringology, Campinas, 3 Department of Childrens Health. University of Missouri, Columbia, USA, 4 Universidad de Valencia, Spain, 5 CUF Tejo Hospital, Lisbon, Portugal; 6 Alicante, Spain, 7 Valencia, Spain, 8 Center of Dental Medicine, Zurich University, Zurich, Switzerland
ABSTRACT
Introduction:
A circadian profile has been suggested in bruxism that may characterize sleep/awake recurrent masticatory muscle activity fluctuations. The current study aims to test whether daylight saving time (DST) as a disruptive factor to the physiologic circadian rhythmicity may affect self-perceived bruxism manifestations.
Methods:
Patients with the criteria for probable bruxism (either awake bruxism or sleep bruxism) were collected from specialized centers in Portugal, Spain, and Brazil. Bruxism symptoms/intensity changes from pre-DST to post-DST implementation were assessed by a questionnaire applied during the week following implementation of DST. Case and control groups (no DST implemented in the country) were compared, and relative frequency of patients reporting changes was computed, and then analyzed using standard statistical approaches.
Results:
A total of 48 patients were included. Circadian distribution of bruxism manifestations varied across the cohort in a symmetric way in cases and control groups. A total of 54.1% of patients and only 18,2% of control patients complained about worsened bruxism symptoms during the week corresponding to the switch to DST (P<0.05). Any of the patients among the cases and 63.6% among the control group reported an improvement of bruxism symptoms after DST/sham treatment.
Discussion:
Preliminary findings are suggestive that bruxism-related symptoms may be affected by the switch to DST, supporting the hypothesis of a sleep-independent circadian role in this condition. Clinical relevance of such findings warrants further confirmation and exploration in future studies.
Keywords:
Daylight Saving Time; Circadian Disruption; Bruxism
Citation:
Meira e Cruz M, Manetta IP, Gozal D, et al. Daylight saving time and self-reported bruxism manifestations: First results from a multicentric, case-control study. J Dent Sleep Med. 2024;11(2)
INTRODUCTION
A circadian bruxism profile has been suggested to characterize sleep/awake recurrent masticatory muscle activity (RMMA) fluctuations. It is, however, unclear whether a true circadian regulation independent of sleep-wake states may contribute to such fluctuations and therefore, whether circadian regulatory factors could explain commonly observed phenotypical differences between patients with bruxism, both from a mechanistic point of view and from a clinical perspective. It is well known that clock genes are expressed in skeletal muscles which are therefore shown to have circadian rhythmicity.1 Further, circadian-mediated changes were shown to be related to fluctuations of human motor activity.2,3 It was also shown that although a small number of expressed genes in skeletal muscle have a circadian rhythm pattern,4 the number of these rhythmic genes depend on the muscle fiber.5 Interestingly, Wolff and colleagues6 argued that scheduled exercise would be able to entrain circadian clocks in skeletal muscles; that is, the phase of rhythmic gene expression and therefore the associated behavior may be associated with the rhythm of locomotor activity. Interestingly, molecular clock also affects muscle phenotype, as described by Kondratov et al.7 Although damage to rhythmic function was shown to affect skeletal muscle phenotype in several clock-related knockout models,8-10 there are no studies assessing whether circadian disruption can affect masticatory muscles and associated activity. Daylight saving time (DST) is an accepted cause of circadian disruption with effect on circadian-modulated systems. Therefore, considering that circadian clocks could have a role in bruxism-associated motor behavior, it can be expected that such behavior would be affected by a circadian challenge as occurring in relation to switching to DST.
The goal of the current study is to test the null hypothesis that self-perceived bruxism manifestation is not affected by DST as a model of circadian disruption.
METHODS
Patients with criteria for probable bruxism (either awake bruxism or sleep bruxism) were collected from three distinct dental sleep/orofacial pain specialized centers in Portugal, Spain (cases) and Brazil (control patients, as DST is absent) during the period of 2022 DST implementation in the European countries involved (the weeks before and after). The clinical coordinator for this study in each center confirmed the criteria applicability and participants were instructed to complete a comprehensive set of guided self-assessment paper-based tools focused on chronotype (Morning- Eveningness Questionnaire), sleep quality (Pittsburgh Sleep Quality Index), and insomnia (Insomnia Severity Index). Although the concept of bruxism remains a controversial issue warranting further clarification, for the purpose of the current study, probable bruxism was interpreted by self-reported symptoms and signs confirmed by the clinical coordinator. Bruxism symptoms/intensity changes from before and after DST implementation were assessed by a brief questionnaire applied the week after DST. The main questions regarding their sleep and bruxism symptoms in the current context were as follows:
(1) "From Saturday to Sunday (beginning of DST) was your sleep different from the usual?” Patients could opt between “No, it was the same”; “Yes, it was worse”; or “Yes, it was better”; (2) If you have bruxism-related symptoms, have they changed after last Saturday? The options were: “No, there were no changes”; “Yes, for worse”; “Yes, for better”. Perception of changes to sleep and bruxism symptoms from before to after DST was therefore addressed and case and control groups were compared. Relative statistical analyses were accomplished using the SPSS statistical software version 23 (IBM Corporation, Armonk, New York, USA). Frequencies (%) were computed for categorical variables and means were calculated for continuous parameters. Differences between groups in categorical parameters were examined using the chi-square test and groups in continuous parameters were assessed by the Mann-Whitney U test.
RESULTS
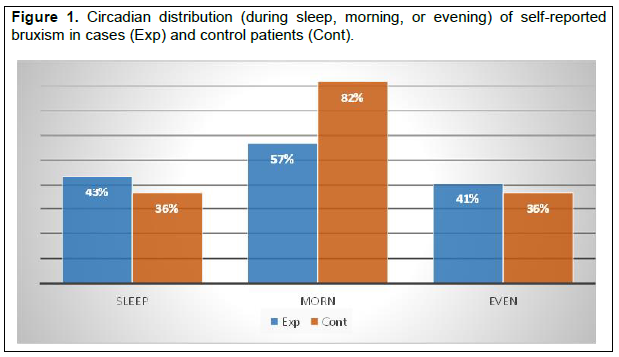
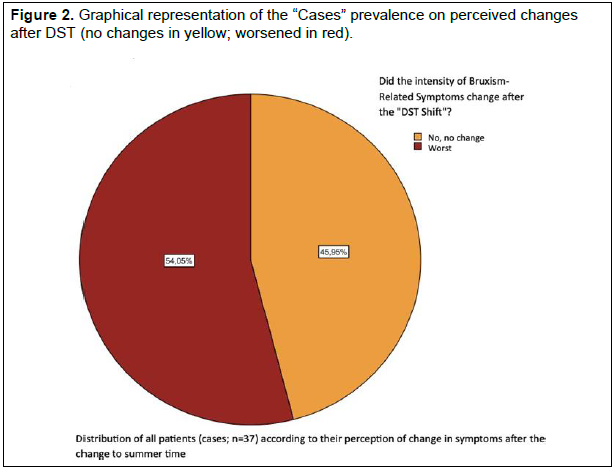
A total of 48 patients (37 cases [16 females] vs 11 controls [32 females]) with a mean age of 42±12.4 years versus 38±12.7 years (P>0.05) were included for analysis. Circadian distribution of bruxism manifestations varied among the sample prevailing in the morning, evening, and during sleep in 57%, 41%, and 43% of the cases and 82%, 36%, and 36% of the control patients. A total of 54.1% of cases versus 18,2% of control patients complained about worsened bruxism symptoms after the switch to DST. Any of the patients among the cases but 63.6% among the control group reported an improvement of bruxism symptoms after DST/sham treatment.
Figure 1Circadian distribution (during sleep, morning, or evening) of self-reported bruxism in cases (Exp) and control patients (Cont). |
{kind=link}
Figure 2Graphical representation of the “Cases” prevalence on perceived changes after DST (no changes in yellow; worsened in red). |
{kind=link}
DISCUSSION
The symmetric distribution of self-reported bruxism manifestations along the 24-hour temporal dynamics observed in this sample corroborate previous findings11 suggesting that circadian clock dynamics parallels functional/parafunctional motor behaviors characterizing bruxism activity, which is in favor of an interaction between both systems. Even though a critical methodologic aspect could conflict with such findings, because often the outcomes of objective and subjective or self-reported assessment tools do not coincide,12 the burden of bruxism may have an effect on sleep medicine clinical practice and should be scrutinized. Interestingly, some studies using “the self-report methodology” also evoked a possible link between bruxism and circadian clocks by evidencing a high prevalence of bruxism complaints in patients with an irregular shift-work schedule.13 It has also previously been documented that sleep-related complaints (37% having trouble falling or staying asleep or sleeping too much), and particularly insomnia (42,6% having moderate to severe levels), are quite prevalent in patients seeking care in a clinical scenario from which bruxism-related behaviors are commonly presented.14 The mechanisms by which such interactions exist are still not established as potential interactors are only poorly described, but stress and coping strategies are believed to be strong contributors.15 However, catastrophic profile may be an important mediator of pain perception in those with sleep bruxism, which in turn seems to align with cognitive behavioral therapeutic strategies.16 Previously published data from Ahlberg and colleagues have also pointed out that individuals with bruxism are frequently burdened by biopsychosocial symptoms, including affective disturbance and early insomnia.17 Also, animal models of musculoskeletal sensitization have been shown to induce disrupted sleep state.18 Although conflicting, recent evidence indicates that at least some phenotypes may account for this mechanism of pain exacerbation associated with bruxism, which may also be aggravated in catastrophic profiles.19 If such a vision is accepted, it is possible that perceived muscular tension or eventually a sequalae from such previous hyperactivity, considering the timeline of the acute events, may contribute to increased sleep latency/insomnia,20 which may also have a catastrophizing profile as a mediator of clinical interest.21 With this hypothesis in mind, it can be expected that patients experiencing bruxism in evening hours close to bedtime would be more prone to experience such sleep onset-related difficulties. Conversely, patients with perceived bruxism manifestations in the morning would be less vulnerable to such consequences. Despite the encouraging results, the current study findings should be interpreted in light of some limitations, such as the code-based diagnosis of bruxism, the unclarified meaning of such repetitive muscular activity within the scope of physiologic/pathophysiologic challenges, and the putative distinct seasonal influence in the cases versus control patients. Even though those aspects would probably not change the main conclusions of this report, they should be targeted in the near future, with controlled studies based on wider samples and eventually different cohorts of patients.
CONCLUSION
These first preliminary results suggest that bruxism symptoms may be affected by the switch to DST, supporting the hypothesis of a sleep-independent circadian role with this condition. Clinical relevance of such findings warrants further exploration in future studies, with additional control of possible confounders and mediators such as psychosocial stress and habits.
REFERENCES
- Zhang R, Lahens NF, Ballance HI, Hughes ME, Hogenesch JB. A circadian gene expression atlas in mammals: implications for biology and medicine. Proc Natl Acad Sci. USA. 2014;111, 16219–16224.
- Dudek M, Meng, QJ. Running on time: the role of circadian clocks in the musculoskeletal system. Biochem J. 2014;463(1):1–8. https://doi.org/10.1042/BJ20140700
- Aoyama S, Shibata S. The role of circadian rhythms in muscular and osseous physiology and their regulation by nutrition and exercise. Front Neurosci. 2017;11:63. https://doi.org/10.3389/fnins.2017.00063
- Miller BH, McDearmon EL, Panda S, et al. Circadian and CLOCK-controlled regulation of the mousetranscriptome and cell proliferation. Proc Natl Acad Sci USA. 2007;104, 3342– 3347. 10.1073/pnas.0611724104
- Dyar KA, Ciciliot S, Tagliazucchi GM, et al. The calcineurin-NFAT pathway controls activity- dependent circadian gene expression in slow skeletal muscle. Mol Metab. 2015;4, 823–833. 10.1016/j.molmet.2015.09.004
- Wolff G, Esser KA. Scheduled exercise phase shifts the circadian clock in skeletal muscle. Med Sci Sports Exerc. 2012;44(9):1663-1670. doi: 10.1249/MSS.0b013e318255cf4c. PMID: 22460470; PMCID: PMC3414645.
- Kondratov RV, Kondratova AA, Gorbacheva VY, Vykhovanets OV, Antoch MP. Early aging and age-related pathologies in mice deficient in BMAL1, the core component of the circadian clock. Genes Dev. 2006;20:1868–1873. 10.1101/gad.1432206
- Dyar KA, Ciciliot S, Wright LE, et al. Muscle insulin sensitivity and glucose metabolism are controlled by the intrinsic muscle clock. Mol Metab. 2015;4, 823–833. 10.1016/j.molmet.2015.09.004
- Schroder EA, Harfmann BD, Zhang X, et al. Intrinsic muscle clock is necessary for musculoskeletal health. J Physiol. 2015;593:5387–5404. 10.1113/jp271436
- Harfmann BD, Schroder EA, Kachman MT, Hodge BA, Zhang X, Esser KA. Muscle-specific loss of Bmal1 leads to disrupted tissue glucose metabolism and systemic glucose homeostasis. Skelet Muscle. 2016;6:12. 10.1186/s13395-016-0082-
- Meira E Cruz M, Winocur E, Gozal D, Lavigne GJ. Chronotype and bruxism: Should we look further and get it from the heart? Cranio. 2021;39(5):457-458. doi: 10.1080/08869634.2021.1956786. PMID: 34369319
- Ohlmann B, Rathmann F, Bömicke W, Behnisch R, Rammelsberg P, Schmitter M. Validity of patient self-reports and clinical signs in the assessment of sleep bruxism based on home-recorded electromyographic/electrocardiographic data. J Oral Rehabil. 2022;49(7):720-728. doi: 10.1111/joor.13327. Epub 2022 Apr 11
- Ahlberg K, Jahkola A, Savolainen A, et al. Associations of reported bruxism with insomnia and insufficient sleep symptoms among media personnel with or without irregular shift work. Head Face Med. 2008;4:4. doi: 10
- Meira E Cruz M, Lukic N, Wojczynska A, Steiger B, Guimarães AS, Ettlin DA. Insomnia in patients seeking care at an orofacial pain unit. Front Neurol. 2019;10:542. doi: 10.3389/fneur.2019.00542. PMID: 31191436; PMCID: PMC6546892.
- Saczuk K, Lapinska B, Wilmont P, Pawlak L, Lukomska-Szymanska M. Relationship between sleep bruxism, perceived stress, and coping strategies. Int J Environ Res Public Health. 2019;16(17):3193. doi: 10.3390/ijerph16173193. PMID: 31480550; PMCID: PMC6747300.
- Ommerborn MA, Depprich RA, Schneider C, Giraki M, Franz M, Raab WH, Schäfer R. Pain perception and functional/occlusal parameters in sleep bruxism subjects following a therapeutic intervention. Head Face Med. 2019;15(1):4. doi: 10.1186/s13005-019-0188-6. PMID: 30696443; PMCID: PMC6350301.
- Ahlberg J, Savolainen A, Rantala M, Lindholm H, Könönen M. Reported bruxism and biopsychosocial symptoms: a longitudinal study. Community Dent OralEpidemiol. 2004;32(4):307-311. doi: 10.1111/j.1600-0528.2004.00163.x. PMID: 15239782.
- Sutton BC, Opp MR. Sleep fragmentation exacerbates mechanical hypersensitivity and alters subsequent sleep-wake behavior in a mouse model of musculoskeletal sensitization. Sleep. 2014;37(3):515-524. doi: 10.5665/sleep.3488. PMID: 24587574
- Baad-Hansen L, Thymi M, Lobbezoo F, Svensson P. To what extent is bruxism associated with musculoskeletal signs and symptoms? A systematic review. J Oral Rehabil. 2019;46(9):845-861. doi: 10.1111/joor.12821. Epub 2019 May 31. PMID: 31090938..1186/1746-160X-4-4. PMID: 18307774; PMCID: PMC2292164.
- Biondi DM. Headaches and their relationship to sleep. Dent Clin North Am. 2001;45(4):685-700. PMID: 11699236.
- Neves LBM, Guimarães AS, Rodrigues LLFR, et al. Self-medication and pain catastrophizing in patients with myofascial pain: Are they related? Oral Dis. 2019;25(6):1672- 1673. doi: 10.1111/odi.13131. Epub 2019 Jun 25.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication April 13, 2023
Submitted in final revised form August 18, 2023
Accepted for publication September 12, 2023
Address correspondence to: Dr. Miguel Meira e Cruz; Address: Sleep Unit, Centro Cardiovascular da Universidade de Lisboa, Lisbon School
of Medicine, Av. Prof. Egas Moniz, 1648-009 Lisbon, Portugal; Email: mcruz@medicina.ulisboa.pt.