Original Article 1, Issue 11.1
Obstructive Sleep Apnea Surveillance and Oral Appliance Therapy Evaluation, Active Duty US Army, 2014-2019
http://dx.doi.org/10.15331/jdsm.7320Christa E. Goodwin, DMD, MS, LTC, USA, DC1, Tyson L. Grier, MS2, Olivia M. Mahlmann, MPH2
1Tri-Service Center for Oral Health Studies, Joint Base San Antonio - Fort Sam Houston, TX 78234, 2 Defense Centers for Public Health-Aberdeen, APG, MD 21010
ABSTRACT
Study Objectives:
Determine the incidence of obstructive sleep apnea (OSA) among United States Army soldiers from 2014 through 2019 and assess self-reported impacts of the disorder and one of its treatments—oral appliance therapy.
Methods:
Surveillance data were obtained from the Armed Forces Health Surveillance Division; remaining data were self-reported through an electronic survey.
Results:
There were 87 404 cases of OSA from 2014 through 2019; incidence rates ranged from 274.3 to 330.3 cases per 10 000 person-years (p-yrs). Male incidence rates (from 294.3 to 355.9/10 000 p-yrs) exceeded female incidence rates (from 155.2 to 189.2/10 000 p-yrs). Soldiers ≥40 years old had the highest incidence rates (from 820.1 to 973.2/10 000 p-yrs). The survey was completed by 8740 soldiers. The majority reported positive airway pressure therapy as their current treatment method; 9% (n=795) reported treatment with an oral appliance. Comparing pretreatment to post-treatment, respondents treated with the oral appliance reported statistically significant improvements in sleep quality, duration, and various aspects of daily life. The predominance (76%) of those treated with anything other than the oral appliance reported they were not aware of the oral appliance as a treatment method.
Conclusions:
Results suggest soldiers are satisfied with the oral appliance; it has significantly improved their sleep quality, duration, and various aspects of daily life.
Clinical Implication:
Military dentists can support a streamlined process to diagnose and treat OSA. The required yearly dental exam provides an opportunity to screen soldiers for OSA and discuss the lesser-known treatment—oral appliance therapy.
Keywords:
obstructive sleep apnea; oral appliance therapy; Army; military; soldiers
Citation:
Goodwin CE, Grier TL, Mahlmann OM. Obstructive sleep apnea surveillance and oral appliance therapy evaluation, active duty US army, 2014-2019. J Dent Sleep Med. 2024;11(1)
INTRODUCTION
Obstructive sleep apnea (OSA), the most common sleep-related breathing disorder, is a rising health concern among the military population.1 Characterized by recurring episodes of upper airway obstruction or narrowing during sleep, OSA is frequently associated with obesity and a large neck circumference.2,3 Troubling comorbidities affiliated with this disorder include hypertension, heart failure, atrial fibrillation, pulmonary hypertension, coronary heart disease, and stroke.2-5 The pathologic process of OSA is rather convoluted as both anatomic and mechanical components contribute to the collapsibility of the upper airway.2 This collapse results in disordered breathing events, including apneas, hypopneas, and respiratory event-related arousals.2-5 Typical signs and symptoms of OSA include excessive daytime sleepiness, loud snoring, gasping, insomnia, and nocturia.2-5
Poor sleep quality introduces various health and safety risks including fatigue, depression, impaired physical and cognitive performance, diminished alertness, and an increased risk of motor vehicle crashes.2,3,5 Considering the high prevalence of OSA, the associated comorbidities and health and safety risks, as well as the accompanying financial implications, this disorder can be considered a significant public health concern.2,3,5
The gold-standard diagnostic test for OSA is an in-laboratory polysomnogram (PSG).2,3,5-8 However, home sleep apnea tests (HSATs) are increasingly being used as they are a more accessible, less costly method for diagnosing OSA in adults.2,3,5-7 The severity of OSA is quantified by the apnea-hypopnea index (AHI)—the number of apneas and hypopneas measured per hour of sleep. Obstructive apneas are characterized by the cessation, or near-cessation, of airflow despite respiratory effort; more specifically, airflow is decreased to less than 10% of the baseline during an obstructive apnea.2,3 Hypopneas, however, are a partial reduction in airflow and further defined as a 30% to 90% airflow reduction.2,3 Consequences of obstructive apneas and hypopneas during sleep include intermittent hypoxemia, changes in intrathoracic pressure, and sleep arousal.2,3 An AHI of less than 5 is considered normal; AHI of 5-14.9 indicates mild OSA; AHI of 15-29.9 is moderate; AHI of 30 or greater indicates severe OSA.2-5
There are a myriad of risk factors for OSA, a major factor being elevated body mass index (BMI),2-3 although, OSA can occur in individuals of normal BMI as well. OSA is most common among men between young adulthood and middle age; however, it can occur at any age, in both males and females. 2-3 Additional risk factors include menopause,enlarged upper airway soft tissues (e.g., tonsils, tongue), and craniofacial abnormalities (e.g., retrognathia). 2-3
The impact of OSA on soldiers and their readiness to deploy is exceptionally relevant, as quality sleep is critical to their mission performance. Treatment options for OSA include positive airway pressure (PAP) therapy, oral appliance therapy, and surgery.2,3,5 Adjunctive behavioral-related interventions include weight loss, exercise, and positional therapy.2,3,5 PAP therapy remains the gold-standard treatment for OSA; however, it requires a great deal of maintenance and can be challenging to adhere to.9 Additionally, deployment to austere locations may make the logistical task of using and maintaining the PAP extremely difficult. Acceptable adherence to PAP therapy is defined as 4 hours of use per night, at least 5 nights per week.3 A 2015 investigation concluded that military personnel with OSA have low adherence to PAP, with 60.3% of study participants found to be nonadherant.9
Oral appliance therapy is an effective treatment for mild and moderate OSA.10-14 Moreover, those suffering from severe OSA have seen improvements in health outcomes while using the oral appliance,14 which is particularly relevant to those intolerant to PAP therapy. This small, lightweight appliance may be a more practical treatment method for soldiers with OSA given the nature of the military profession; it presents with an ease of use that can improve soldier readiness.
This project serves as both a surveillance and treatment method evaluation. The purpose is 3-fold: determine the incidence of OSA among active duty US Army soldiers from 2014 through 2019; assess the identified soldiers’ subjective, self-reported impacts of this disorder and one of its treatment methods—oral appliance therapy; and assess soldiers’ compliance and satisfaction with the oral appliance.
METHODS
The US Army Public Health Center (APHC), currently named the Defense Centers for Public Health-Aberdeen, approved this surveillance evaluation and survey as public health practice; it was assigned project #19-744.
Surveillance
The surveillance data were obtained from the Armed Forces Health Surveillance Division (AFHSD). Data analyses were restricted to active duty Army soldiers diagnosed with OSA from 2014 through 2019. The following case definition was developed by AFHSD for the purpose of epidemiological surveillance:
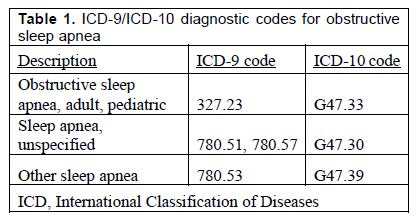
- One hospitalization with any of the defining diagnoses of OSA (Table 1) in any diagnostic position; or
- Two outpatient medical encounters within 90 days of each other, with any of the defining diagnoses of OSA (Table 1) in any diagnostic position.
- The incident date was considered the date of the first hospitalization or outpatient medical encounter that included a defining diagnosis of OSA.
- An individual was considered an incident case only once per lifetime.
Analysis of surveillance data was conducted using Microsoft Excel 2016. Yearly incidence rates were estimated by dividing the number of incident diagnoses by the number of active duty Army soldiers reported in the Defense Medical Epidemiology Database (DMED) for that particular year. Incidence rates were further stratified by sex, age group, and rank.
A discrepancy was found in the surveillance data following the initial stages of analysis. An inconsistency in the number of identified cases led to a reinvestigation of the data requisition. It was determined that the incidence rule listed above (once per lifetime) was not initially taken into account by AFHSD. As such, prevalent cases were not excluded, and our case list consisted of some individuals initially diagnosed with OSA prior to the surveillance period (2014-2019). This affected our survey population, as the survey was distributed prior to identifying this problem.
A new data requisition, including the ‘once per lifetime’ incidence rule, was completed; the surveillance findings presented below reflect this. Following a cross-reference of the survey respondents’ identities with the list of cases, it was determined that 15% (n=1307) of the survey respondents were soldiers initially diagnosed with OSA prior to 2014. Soldiers’ self-reported impacts of this disorder and its treatment are extremely relevant to the Army, regardless of the diagnosis year. Accordingly, it was decided that all feedback should be included in this report.
Survey
The survey was published in Verint, a secure electronic survey platform. Email addresses for soldiers diagnosed with OSA during the surveillance period were obtained from the Defense Manpower Data Center (DMDC). The intent was to electronically distribute the survey to all previously identified soldiers; however, email addresses were only available in DMDC for 34% (n=37 162) of the identified soldiers. On 30 September 2020, an email containing the link to the survey was sent to the 37 162 soldiers. Over the next several months, soldiers who had not yet completed the survey received email reminders. The survey closed on 28 December 2020.
The survey began with three exclusion questions; it immediately ended for those who did not consent, reported they were no longer active duty, or reported they were not diagnosed with OSA during the specified time frame (2014-2019). Next, demographics including age, sex, rank, and military occupational specialty were obtained. In addition, soldiers were asked to report physical characteristics (height, weight), OSA severity, deployment eligibility, OSA treatment method(s) discussed with provider(s), and current OSA treatment method(s).
The most effective treatment plans for managing OSA and other sleep-related breathing disorders are multidisciplinary and comprehensive.11 Therefore, soldiers had the option to select multiple methods. Soldiers who reported treatment with anything other than the oral appliance were asked if they were aware of oral appliance therapy prior to taking the survey.
The following section gave soldiers the opportunity to rate the impact of OSA on several subjective measures of everyday wellness (measured on a 5-point Likert scale) prior to initiating any form of treatment, including sleep quality and duration, daily performance, cognitive level, alertness, level of physical activity, fatigue, and daytime sleepiness. The survey ended for those who reported treatment with any method other than the oral appliance. For soldiers who reported treatment with the oral appliance (either exclusively, or in conjunction with other treatment modalities) the survey continued with an evaluation of treatment compliance and satisfaction. Soldiers were again asked to rate the impacts on everyday wellness (sleep quality and duration, cognition, alertness, physical activity, daytime sleepiness, etc.); however, they were instructed to consider the impact post-treatment with the oral appliance for at least 1 month. The period of 1 month was selected because the oral appliance may require some adjustments in the first few weeks following delivery.
At the time this study took place, there was no standardized definition of oral appliance adherence within the dental sleep medicine community.15 A definition for adherence was established specifically for this study. Adherence was defined as wearing the oral appliance for at least 80% of an average night of sleep, calculated by dividing the reported average number of hours the oral appliance was worn per night by the reported average number of hours slept per night. Adherence did not consider the reported number of nights per week the oral appliance was used. This is because in the open-ended question of the survey, numerous soldiers indicated that the oral appliance was used as an ‘alternate therapy’ when deployed (or traveling), as they were unable to use the CPAP in those environments due to unreliable electricity and/or inability to obtain maintenance supplies, for example.
Data analyses were conducted using SPSS Version 21.0 and Open Source Epidemiologic Statistics for Public Health, Version 3.01. Missing or invalid responses were excluded. Means and standard deviations for height and weight were calculated and stratified by sex. BMI was calculated based on the height and weight reported at the time the survey was taken, not at the time of disorder diagnosis. The following formula was used: (weight (lb) ÷ height (in) 2)*703. Frequencies were calculated by sex for the following: age, BMI, rank, disorder severity, deployment eligibility, treatment method(s) discussed with provider(s), current treatment method(s), and awareness of the oral appliance prior to taking survey. Soldiers who reported any airway pressure device as current method of treatment were included in the ‘PAP therapy’ group for all analyses. These devices included the following: continuous positive airway pressure (CPAP), average volume-assured pressure support (AVAPS), autoadjustable positive airway pressure (APAP), adaptive servo-ventilation (ASV) device, and bilevel positive airway pressure (BiPAP).
Shapiro-Wilk normality tests were conducted, indicating that the data were not normally distributed; nonparametric tests were thus used for subsequent analysis of the survey data. Wilcoxon signed-rank tests were used to evaluate differences in pretreatment to post-treatment variable ratings by sex and reported treatment method. Pretreatment to post-treatment comparisons were made among several different groups of soldiers based on reported treatment method(s), including those treated with both the oral appliance and PAP therapy, those treated exclusively with the oral appliance, and those treated with the oral appliance (either exclusively or in combination with any other method). Results of all comparisons can be found in the full technical report approved by the APHC and published on the Defense Technical Information Center—Technical Report No. S.0079064.3-21.16 However, this specific publication focuses only on the comparisons made among the latter group of soldiers (i.e., soldiers who reported treatment with the oral appliance, either exclusively or in combination with any other method). Consistent with convention, an alpha level of .05 was used as the cut off for defining statistical significance, (i.e., P ≤ .05).
There were no pretreatment to post-treatment comparisons made among soldiers who did not report treatment with the oral appliance. The purpose of this evaluation was not to compare the oral appliance to PAP therapy, or to any other treatment method. For this reason, those who reported a treatment other than the oral appliance received a shortened survey.
RESULTS
Surveillance
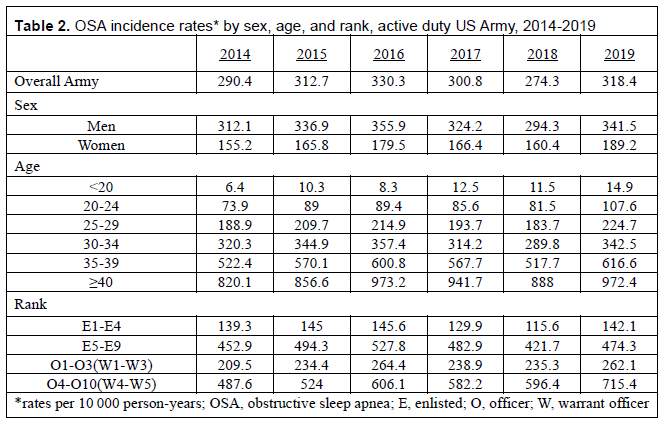
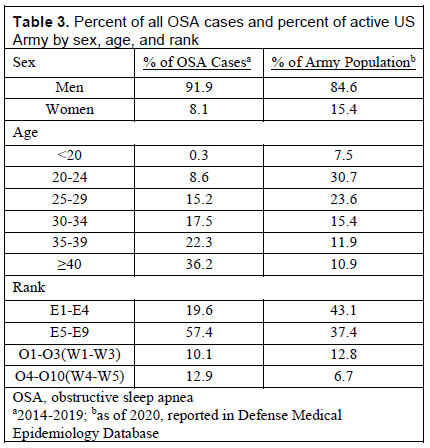
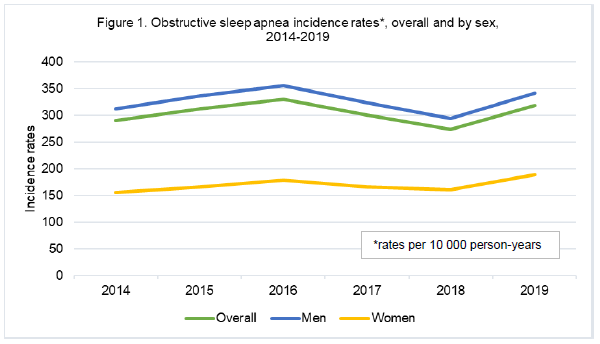
There were 87 404 incident diagnoses of OSA among active Army soldiers from 2014 through 2019. Incidence rates for the Army overall and by sex are illustrated in Figure 1. Table 2 lists incidence rates of OSA by year, sex, age, and rank. Yearly incidence rates for the Army overall ranged from 274.3 to 330.3 cases per 10 000 p-yrs. The number of male cases (n=80 323) far exceeded that of female cases (n=7081). Male incidence rates (from 294.3 to 355.9 cases per 10 000 p-yrs) also exceeded that of females (from 155.2 to 189.2 cases per 10 000 p-yrs). Men comprised 91.9% of all OSA cases during this study period, and as of 2020, 84.6% of the Army (Table 3).
The greatest proportion (36.2%) of all OSA cases occurred among soldiers ≥40 years of age. As of 2020, this age group comprised the smallest proportion (10.9%) of the Army (Table 3). Soldiers ≥40 years of age had the highest incidence rates of any other age group (from 820.1 to 973.2 cases per 10 000 p-yrs); Soldiers ≤20 years of age had the lowest rates (from 6.4 to 14.9 cases per 10 000 p-yrs) (Table 2).
The greatest proportion (57.4%) of all OSA cases occurred among soldiers in the ranks of E5-E9 (Table 3). As of 2020, those in the ranks of O4-O10 comprised the smallest proportion (6.7%) of the active Army yet had the highest incidence rates (from 487.6 to 715.4 cases per 10 000 p-yrs) (Table 2). Soldiers in the ranks of E1-E4 had the lowest incidence rates ranging from 115.6 to 145.6 cases per 10 000 p-yrs.
Survey
The survey was sent electronically to 37 162 soldiers; email addresses for all identified cases could not be located. The survey was initiated by 12 090 soldiers for an initial response rate of 33%. However, the survey was not completed by all who initiated it. Those who answered ‘No’ to one or more of the exclusion questions were immediately excluded, as were soldiers who exited prior to completing the entire survey. The final number of soldiers who submitted the survey totaled 8740 (24%).
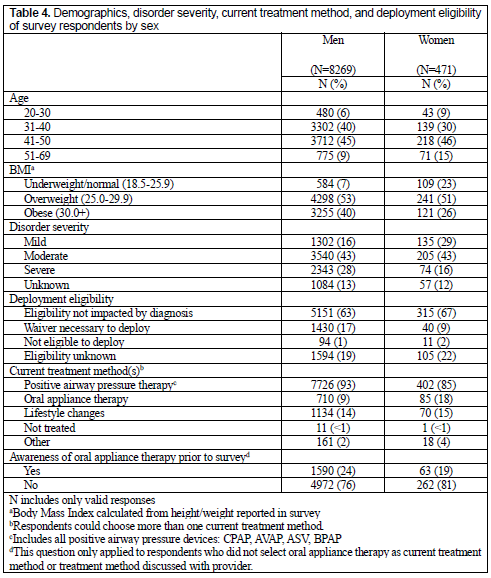
Table 4 displays the reported demographics, OSA severities, deployment eligibilities, and treatment methods of survey respondents. The majority of survey respondents were men (95%; n=8269) between 41 and 50 years of age (45%; n=3930) in the enlisted (E) ranks of E4 through E9 (63%; n=5469). Fifty-three percent (n=4298) and 51% (n=241) of male and female survey respondents, respectively, were considered overweight; 40% (n=3255) and 26% (n=121) were considered obese. The vast majority (93%; 402 women, 7726 men) reported treatment with PAP therapy, either in combination with other treatment modalities, or exclusively. Nine percent of soldiers (n=795; 85 women, 710 men) reported treatment with the oral appliance. Of these soldiers treated with the oral appliance, 45% (n=360; 41 women, 319 men) were treated with it exclusively; the remaining reported a combination of the oral appliance and other treatment modalities (e.g., PAP therapy, lifestyle changes, medication, etc.). The majority (76%; n=5234) of soldiers who reported treatment with anything other than the oral appliance reported they were not aware of oral appliance therapy as a treatment for OSA prior to taking the survey.
The majority (43%) of respondents reported moderate OSA. Twenty-eight percent reported severe OSA; 13% were unaware of the severity of their disorder. The great majority of survey respondents (63%, n=5466) indicated that deployment eligibility was not impacted by disorder diagnosis; 16% (n=1470) reported that a waiver was required for deployment. Of the soldiers who reported treatment with the oral appliance, 88% were considered adherent to the treatment; adherence among men (88%) was equal to that of women (88%).
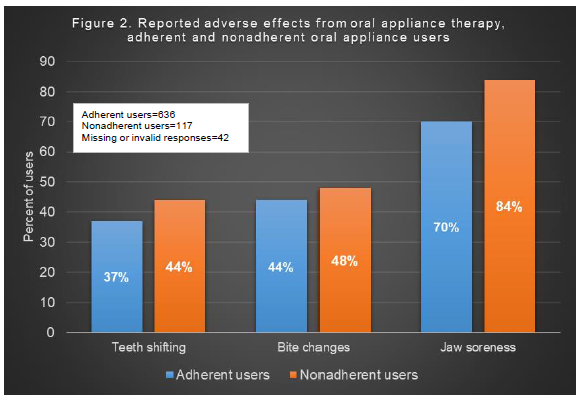
Figure 2 illustrates the proportion of adherent and nonadherent oral appliance users who reported adverse effects (teeth shifting, bite changes, jaw soreness) following treatment. A greater proportion of nonadherent users reported teeth shifting, bite changes, and jaw soreness compared to adherent users. The most common reported adverse effect, reported by 70% of adherent oral appliance users and 84% of nonadherent users, was jaw soreness.
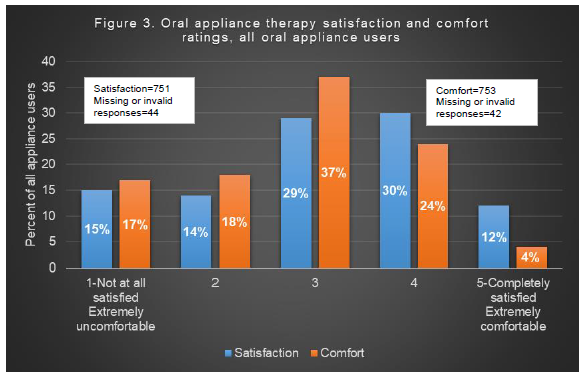
Figure 3 illustrates oral appliance overall satisfaction and comfort ratings of all soldiers treated with the appliance, regardless of adherence. On a scale of 1 to 5 (1-not at all satisfied; 5-completely satisfied), 29% (n=218) of soldiers rated satisfaction as 3; 30% (n=221) rated satisfaction as 4. On a scale of 1 to 5 (1-extremely uncomfortable; 5-extremely comfortable), 37% (n=280) rated comfort as 3; 24% (n=177) rated it as 4.
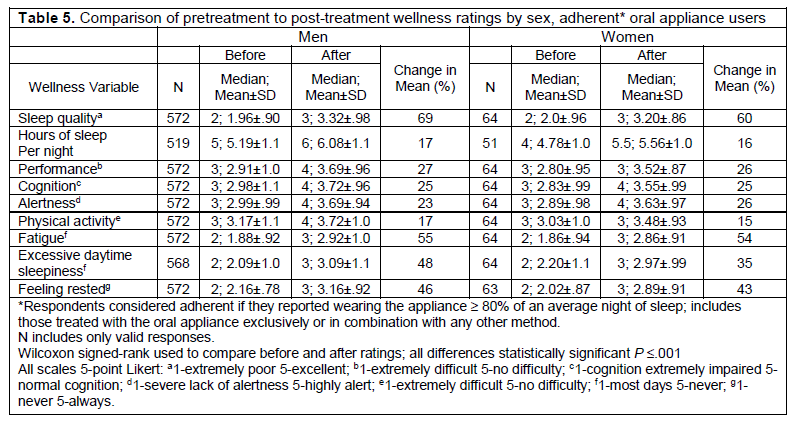
Table 5 displays the pretreatment to post-treatment comparisons of male and female soldiers adherent to the oral appliance. All soldiers reported statistically significant improvements (P ≤ .001) in all wellness variables (sleep duration and quality, cognition, alertness, physical activity, fatigue, etc.). The wellness variable with the greatest percent improvement among both men and women was sleep quality (69% for men, 60% for women). The variable with the lowest percent of improvement among women was physical activity (15%); among men, both sleep duration (17%) and physical activity (17%) had the lowest percent of improvement.
At the conclusion of the OSA survey, soldiers were presented with an open-ended question that provided them the opportunity to share any additional information they chose regarding their experiences, diagnoses, treatments, etc. Many soldiers (n=1280) took advantage of this opportunity and chose to provide very lengthy comments. However, the discussion of these comments, including their relevance, deserves more space than permitted in this publication. Therefore, the open-ended comments will be reviewed and discussed at length in a separate commentary report. Alternatively, they can be reviewed in the APHC Technical Report No. S.0079064.3-21.16
Table 1ICD-9/ICD-10 diagnostic codes for obstructive sleep apnea |
{kind=link}
Table 2OSA incidence rates* by sex, age, and rank, active duty US Army, 2014-2019 |
{kind=link}
Table 3Percent of all OSA cases and percent of active US Army by sex, age, and rank |
{kind=link}
Table 4Demographics, disorder severity, current treatment method, and deployment eligibility of survey respondents by sex |
{kind=link}
Table 5Comparison of pretreatment to post-treatment wellness ratings by sex, adherent* oral appliance users |
{kind=link}
Figure 1Obstructive sleep apnea incidence rates*, overall and by sex, 2014-2019 |
{kind=link}
Figure 2Reported adverse effects from oral appliance therapy, adherent and nonadherent oral appliance users |
{kind=link}
Figure 3Oral appliance therapy satisfaction and comfort ratings, all oral appliance users |
{kind=link}
DISCUSSION
Surveillance
OSA constitutes a significant burden to our soldiers, with 87 404 diagnoses from 2014 through 2019. The year-to-year incidence rates exhibited minor fluctuations during this period; however, there has been a considerable rise in OSA diagnoses over the last 15 years.1,17 According to one study,1 the incidence of OSA among active US Army soldiers increased 600% from 2004 to 2013. Likewise, the percentage of those classified as overweight or obese has been increasing throughout the years. In a study of active duty personnel, the combined overweight and obesity prevalence increased from 50.6% in 1995 to 60.8% in 2008.18 Additionally, an investigation of Army recruits showed a 19% increase in BMI among both men and women from 1975 to 2013.19 The increase in overweight and obese soldiers may have contributed to the increase in OSA diagnoses throughout the years. Furthermore, a greater awareness of this disorder, its symptoms, and its risk factors may have led to a greater number of PSG referrals, and ultimately a greater number of diagnoses.
OSA is more common among men, both in the general population and active Army. The vast majority of the cases (92%) were among male soldiers. Given the gender distribution in the Army, this is to be expected. Nevertheless, when assessing risk, male soldiers consistently had higher incidence rates compared to female soldiers. OSA is a result of upper airway collapse during sleep. It has been suggested that the higher prevalence of OSA among men may be attributed to the sex-related differences in the structure and physiological behavior of the upper airway.20 Literature shows that women have augmented genioglossal muscle activity compared to men, as well as a different upper airway shape.20 This increased activity results in greater upper airway stability, making upper airway closure during sleep less likely.20
In the general population, OSA is most commonly diagnosed between young adulthood and middle age. The vast majority of active duty Army soldiers (89%) are 39 years of age or younger. Soldiers 40 years or older comprise the smallest proportion of the Army (11%), yet this age group experienced the greatest proportion of cases (36%) and the highest incidence rates. Therefore, while the preponderance of active Army soldiers is under the age of 40, those over 40 have a substantially higher risk of OSA diagnosis. As discussed previously, obesity is a major risk factor for OSA. Consequently, the sex and age distribution of obesity among active Army soldiers is highly relevant when considering the sex and age distribution of OSA among active Army soldiers. The last three iterations of the APHC’s Health of the Force Report21-23 stated that 17% of active Army soldiers were obese; the prevalence of obesity increased with age, and in all age groups men were more likely to be obese than women. Therefore, the higher rates of OSA among older male soldiers may be associated with the higher likelihood of obesity among this group.
As of 2019, enlisted soldiers represented the vast majority of the Army (80%); predictably, this group represented the greatest proportion of OSA diagnoses during this study period (77%). However, when considering risk, officers in the ranks of O4 through O10 had the highest incidence rates. This greater risk may be attributed to the differing age distributions among ranks. As of 2020, almost a third (29%) of officers were 40 years or older, while only 7% of enlisted soldiers were in this age group.
Survey
Follow-up PSGs are very useful for determining the efficacy of treatment (i.e., how well it works under ideal, controlled conditions). However, they do not measure the treatment’s effectiveness (i.e., how well it performs in real-world conditions). Therefore, this survey was designed to assess soldiers’ subjective, self-reported impacts of OSA and oral appliance therapy, as well as their compliance and satisfaction with this treatment. The initial survey response rate of 33% suggests that OSA is an important concern among soldiers.
Considering the longevity and proven efficacy of PAP therapy, it was not surprising that the vast majority of soldiers reported treatment with the PAP device. However, the responses in the open-ended question indicated that some soldiers alternate treatment methods (i.e., use of PAP therapy at home and oral appliance during deployments or when traveling), while others use them in conjunction. This is not unusual, as alternating treatments may help minimize adverse effects of either therapy.
Deployment Eligibility and OSA Severity
According to the minimum standards of fitness for deployment,24 soldiers with moderate to severe OSA require waivers to deploy, yet the majority of survey respondents (63%) indicated that deployment eligibility was not impacted by OSA diagnosis. However, a soldier may not be aware of deployment eligibility until the time he/she is assigned to deploy.
OSA severity was self-reported and unable to be validated, a distinct limitation of this study. Similar to deployment eligibility, soldiers may not be aware of the severity of their disorder, as it is based on the AHI index measured during the PSG. Some likely assessed the severity of their disorder based on their subjective view of the severity of the impact on day-to-day life.
Adherence
The vast majority (88%) of oral appliance users were considered adherent to the treatment. However, it must be reiterated that the determination of adherence included the use of a definition constructed specifically for this investigation.
Adherence to treatment may be affected by a multitude of factors, including adverse effects experienced, as well as overall comfort and satisfaction with the treatment. The majority of oral appliance users rated overall appliance satisfaction as 4 (1-not at all satisfied; 5-completely satisfied); the majority rated overall appliance comfort as 3 (1-extremely uncomfortable; 5-extremely comfortable). Although, when assessing adverse events by treatment adherence, a greater proportion of nonadherent soldiers reported adverse events from the appliance (teeth shifting, bite changes, and jaw soreness) compared to adherent soldiers. This finding is to be expected, as patients experiencing adverse effects from a prescribed treatment would be less likely to comply with it
Pretreatment to Post-Treatment Wellness Comparisons
This report focuses on all soldiers treated with the oral appliance, exclusively or in combination with other treatments. The results of this survey demonstrate that the oral appliance has significantly improved their sleep quality and duration, as well as other wellness-related aspects of daily life (e.g., alertness, cognition, daily performance, etc.). However, in our complete investigation,16 those treated exclusively with the oral appliance were separated from those treated with both the PAP device and oral appliance. Similar results were found; both groups reported statistically significant improvements in all wellness variables pretreatment to post-treatment.16 However, when observing the percent change in the wellness ratings pretreatment to post-treatment, the improvement was greater for those treated with the oral appliance and PAP, compared to those treated exclusively with the oral appliance.16 These findings suggest that combination therapy may provide more relief than just the oral appliance alone.16 However, whether or not those treated with both the oral appliance and PAP therapy alternated the treatments or used them in conjunction is unknown.
Awareness
The first modern oral appliances for treating OSA were developed in 1982.25 Despite the fact that oral appliance therapy is not a newly developed treatment method, for many years it has been underused compared to PAP therapy, most likely due to lack of awareness. The vast majority (76%, n=5234) of soldiers who reported any treatment method other than the oral appliance indicated they were not aware of this treatment prior to taking the survey. Perhaps some medical providers do not discuss oral appliance therapy with soldiers because they themselves are not aware of it, or they do not believe it is an effective method for treating this disorder. Nevertheless, the oral appliance may gain more attention since Philips Respironics, a principal military PAP device supplier, recently issued a device recall.26 This recall notification was released 4 months after the close of the survey. Therefore, the specific impact the recall had and continues to have on soldiers suffering from OSA is unknown at this time.
Military dentists have an opportunity to support a streamlined process to diagnose and treat OSA. While a dentist cannot officially diagnose this disorder, the required yearly dental exam provides the dentist with the opportunity to screen soldiers for it. Additionally, the information that is routinely gathered during comprehensive dental examinations (e.g., health of hard and soft tissues of the mouth, location and integrity of teeth, etc.) will help determine if a patient is a candidate for the oral appliance, should that patient be diagnosed with OSA in the future. The creation of this collaborative nature between dentists and physicians will serve to simplify and improve the OSA diagnostic and treatment processes.
The Defense Health Agency’s (DHA) Quadruple Aim is improved readiness of the force through better health, better care, at lower cost.27 Oral appliances are much less expensive to provide compared to a PAP device.12 A recent study12 outlined the potential cost savings for the military that oral appliance therapy offers. There were roughly 4800 oral appliances issued Army-wide between August 2016 and August 2020 costing $2.1 million.12 Had the PAP device been issued to those patients instead of the oral appliance, the cost would have been $4.8 million.12 Ultimately, oral appliance therapy aligns with the DHA’s Quadruple Aim by successfully treating OSA, thereby improving readiness and deployability, at a lower cost.12,27
Limitations
The use of ICD diagnostic codes for surveillance studies, in any position, comes with limitations. These codes may not always translate into an official diagnosis. This was evident once the survey was administered to the soldiers who were previously identified as OSA cases. Numerous soldiers (n=71) responded to the survey via email indicating they did not have OSA. Some reported they had been tested for it in the past, after which they were informed that they did not have OSA. Some soldiers indicated they were diagnosed with other sleep-related disorders (e.g. restless leg syndrome, insomnia, etc.), while others reported that if they did in fact have OSA, they were never informed of it. When these 71 soldiers were cross-referenced with the list of cases provided by AFHSD, it was determined that 18% of them did not display the OSA diagnostic code in the primary diagnostic position, but instead in a higher position (i.e., second through fourth positions). Therefore, the position of the ICD code may be of relevance when attempting to determine the true incidence (or prevalence) of a medical disorder or disease.
Self-reported studies, in general, present multiple validity problems including the following: respondents may exaggerate symptoms, they may underreport or over-report frequencies, or they may simply misremember specific details. Therefore, while it was very important to capture soldiers’ subjective, self-reported burdens of this disorder, and their comfort and satisfaction with treatment, the confines of this specific type of study are well recognized and appreciated.
CONCLUSIONS AND RECOMMENDATIONS
Quality sleep is critical to mission readiness. It is a valuable contributor to mental and physical health and provides the body with an opportunity to restore and rejuvenate itself. Consequences of poor sleep quality include emotional distress, impaired cognition, risk of injury, and multiple other short- and long-term health complications.2-5 Unfortunately, sleep-related breathing disorders among soldiers are not uncommon.1,16, 21-23 Additionally, the nature of the profession presents many sleep-related challenges.
This study demonstrates that OSA remains a prevalent disorder, notably among older Army soldiers. To our knowledge, this is the first survey assessing soldiers’ subjective burdens from this sleep disorder, as well as their compliance and satisfaction with oral appliance therapy. The efficacy of PAP therapy has been thoroughly studied and proven; it remains the gold-standard treatment. However, it is expensive, requires a great deal of maintenance, and can be challenging to adhere to.9 For many, PAP therapy is difficult to adhere to under ideal circumstances; in a deployed environment, its use can be thoroughly burdensome and inconvenient. Oral appliance therapy is an effective treatment that can be used as an alternative to, or in conjunction with, PAP therapy.10-14 The oral appliance is small, lightweight, and requires no electricity. Its ease of use, particularly in austere locations, provides it with the ability to improve soldier readiness.
This survey indicates that overall, soldiers are satisfied with oral appliance therapy. Additionally, this treatment significantly improved their sleep quality, duration, and various aspects of daily life. It was noteworthy to discover that the vast majority of soldiers managed by methods other the oral appliance were not aware of the oral appliance as a treatment method for OSA. This finding in addition to the multitude of comments recounting the struggles of receiving a diagnosis and effective treatment indicate some barriers within the military health care system exist.16 Consequently, an assessment of the current processes for screening, diagnosis, and treatment of soldiers with sleep-related breathing disorders is well founded. Army dentistry has the opportunity to support Army medicine in the streamlining of these processes. Ultimately, evaluation of long-term oral appliance therapy outcomes and cost-savings analyses may benefit the military and soldiers with OSA.
DISCLAIMER
The views expressed in this publication are those of the authors and do not necessarily reflect the official policy or position of the Department of the Army, the Department of Defense, or the US Government. The mention of any non-federal entity and/or its products is for informational purposes only, and not to be construed or interpreted, in any manner, as federal endorsement of that non-federal entity or its products.
REFERENCES
Rogers A, Stahlman S, Hunt D, Oh G, Clark L. Obstructive sleep apnea and associated attrition, active component, U.S. Armed Forces, January 2004-May 2016. MSMR.2016; 23(10): 2-11.
Kryger M, Roth T, Goldstein C, Dement W. Principles and Practice of Sleep Medicine. 7th edition. Elsevier; 2022.
Gottlieb DJ, Punjabi NM. Diagnosis and Management of Obstructive Sleep Apnea: A Review. JAMA. 2020 Apr 14;323(14):1389-1400.
Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014 Nov; 146(5):1387-1394.doi:10.1378/chest.14-0970
Das A, Chang J, Berneking M, Hartenbaum N, Rosekind M, Gurubhagavatula I. Obstructive sleep apnea screening, diagnosis, and treatment in the transportation industry. J Clin Sleep Med. 2022;18(10):2471–2479.
Caples S, Anderson W, Calero K, Howell M, Hashmi S: Use of polysomnography and home sleep apnea tests for the longitudinal management of obstructive sleep apnea in adults: an American Academy of Sleep Medicine clinical guidance statement. J Clin Sleep Med. 2021; 17: pp. 1287-1293. doi:10.5664/jcsm.9240
Kapur V, Auckley D, Chowdhuri S, Kuhlmann D, Mehra R, Ramar K, Harrod C. Clinical practice guideline for diagnostic testing of adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. JCSM. 2017;13(3): 479-504.
Rundo JV, Downey R. Polysomnography. Handb Clin Neurol.2019; 160:381-392.
Mysliwiec V, Capaldi V, Gill J, Baxter T, O’Reilly B, Matsangas P; Roth B. Adherence to positive airway pressure therapy in the U.S. military personnel with sleep apnea improves sleepiness, sleep quality, and depressive symptoms. Military Medicine. 2015;180(4):475-482.
Lettieri CJ, Paolino N, Eliasson AH, Shah AA, Holley AB. Comparison of adjustable and fixed oral appliances for the treatment of obstructive sleep apnea. J Clin Sleep Med. 2011;7(5):439-445.
Levine M, Bennett K, Cantwell M, Postol K, Schwartz D. Dental sleep medicine standards for screening, treating, and managing adults with sleep-related breathing disorders. JDSM. 2018;5(3). http://dx.doi.org/10.15331/jdsm.
Knowles S, Dekow M, Williamson M. Oral appliances for OSA treatment: meeting the quadruple aim. Military Medicine. 2023;188(3-4):e718-e724. https://doi.org/10.1093/milmed/usab316
Lim J, Lasserson T, Fleetham J, Wright J. Oral appliances for obstructive sleep apnea. Cochrane Database Syst Rev. 2006; 25(1):CD004435
Sutherland K, Phillips C, Cistulli P. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: cpap and oral appliances. JDSM. 2015; 2(4):175-181
Radmand R, Chiang H, Giosia M, Galang-Boquiren M, Rohatgi R, Silk D, Vanderveken O, Adame M. Defining and measuring compliance with oral appliance therapy. JDSM. 2021;8(3). http://dx.doi.org/10.15331/jdsm.
Goodwin CE, Grier TL, Mahlmann OM. U.S. Army Public Health Center Technical Report No. S.0079064.3-21: Obstructive Sleep Apnea Surveillance and Oral Appliance Therapy Evaluation, Active Duty U.S. Army, 2014-2019. Defense Technical Information Center, https://iscover.dtic.mil/, AD1171341. May 2022
Caldwell J, Knapik J, Shing T, Kardouni J, Lieberman H. The association of insomnia and sleep apnea with deployment and combat exposure in the entire population of US Army soldiers from 1997 to 2011: a retrospective cohort investigation. Sleep. 2019; 42(8):zsz112. doi:10.1093/sleep/zsz112
Reyes-Guzman C, Bray R, Forman-Hoffman V, Williams J. Overweight and obesity trends among active duty military personnel, a 13-year perspective. Am J Prev Med. 2015; 48(2):145-153. doi:10.1016/j.amepre.2014.08.033
Knapik JJ, Sharp MA, Steelman RA. Secular trends in the physical fitness of United States Army Recruits on entry to service, 1975-2013. J Strength Cond Res. 2017; 31(7):2030-2052. doi:10.1519/JSC.0000000000001928
Schwab R. Sex differences and sleep apnoea. Thorax. 1999;54:284-285. doi:10.1136/thx.54.4.284
Health of the Force (2018).U.S. Army Public Health Center https://phc.amedd.army.mil/Periodical%20Library/2018HealthoftheForceReport.pdf
Health of the Force (2019). U.S. Army Public Health Center https://phc.amedd.army.mil/PHC%20Resource%20Library/2019_Health-of-the-Force.pdf
Health of the Force (2020). U.S. Army Public Health Center https://phc.amedd.army.mil/PHC%20Resource%20Library/2020-hof-report.pdf
United States Central Command. USCENTCOM. Modification Seventeen (Tab A): Amplification of the Minimal Standards of Fitness for Deployment to the CENTCOM AOR; to Accompany Modification Seventeen to USCENTCOM Individual Protection and Individual/Unit Deployment Policy, https://www.centcom.mil/Portals/6/MEDICAL/MOD17_Tab_A.pdf
Demko B. The history behind the mechanics of oral appliance therapy for the treatment of obstructive sleep apnea. JDSM. 2019;6(1).
Philips Corporation. Voluntary Recall Information: Philips Respironics Sleep and Respiratory Care devices. Philips Respironics, 14 June 2021. Updated: December 7, 2023. https://www.usa.philips.com/healthcare/e/sleep/communications/src-update
Health.Mil. MHS Quadruple Aim. The Defense Health Agency. August 23, 2017. https://www.health.mil/Reference-Center/Glossary-Terms/2017/08/23/MHS-Quadruple-Aim
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted September 20, 2022
Submitted in final revised form April 12, 2023
Accepted for publication May 15, 2023
Address correspondence to: LTC Christa E. Goodwin, DMD, MS. Email: christa.goodwin@usuhs.edu