Original Article 1, Issue 1.1
Sleep Medicine Education at Dental Schools in Australia and New Zealand
http://dx.doi.org/10.15331/jdsm.3728
Ramesh Balasubramaniam, BDSc, MS1 ; Andrew Pullinger, DDS, MSc2 ; Michael Simmons, DMD, FAGD3
1 School of Dentistry, University of Western Australia, Perth, Western Australia, Australia; 2 University of California, Los Angeles, School of Dentistry, CA; 3 University of California, Los Angeles, School of Dentistry, Clinical Assistant Professor, Ostrow School of Dentistry, Los Angeles, CA
ABSTRACT
Background:
Traditionally, the curriculum in Australian and New Zealand dental schools has largely ignored the need for future dentists to receive foundational education in the field of sleep medicine. The absence of official education accreditation standards means this increasing part of dental practice continues as a continuing education activity without proper accountability by organized dentistry. This manuscript evaluates the current status of education in sleep disorders to predoctoral dental students.
Methods:
All 10 dental schools in Australia and New Zealand were surveyed for information regarding their sleep medicine curriculum during the 2011 academic year. The head of each dental school or relevant course coordinator responded to a questionnaire.
Results:
One dental school did not respond, and 3 dental schools were unable to complete the survey, as they had not graduated a class. Therefore 6 of the potential 7 dental schools (85.7%) completed the survey. The average total predoctoral sleep medicine teaching time was 4.5 hours (SD 2.51; range 2 to 8 h). Five of the 6 dental schools spent most of their sleep medicine curriculum time teaching in the fifth year of 5-year programs (mean of 2.5 h; SD 2.88). Education time spent in sleep medicine was 55% didactic. All responding dental schools reviewed obstructive sleep apnea, 83% reviewed sleep bruxism, and 67% reviewed primary snoring.
Conclusions:
Although a definite beginning, current sleep medicine education at Australian and New Zealand dental schools still seems to be at an exposure level, and likely inadequate for competency in screening for sleep related breathing disorders as the primary requirement. It also seems to be minimal foundation for participating as a future dentist member of the sleep medicine team, which with further post graduation training may include providing oral appliance therapy for sleep disordered breathing when appropriate. This appears to be a similar outcome to the level of education in sleep medicine provided in the United States dental school predoctoral programs to date.
Keywords:
sleep medicine education, sleep disordered breathing, competency, dental sleep medicine
Citation:
Balasubramaniam R, Pullinger A, Simmons M. Sleep medicine education at dental schools in Australia and New Zealand. Journal of Dental Sleep Medicine 2014;1(1):9–16.
The field of dental sleep medicine (DSM) has become an area of importance for comprehensive dental education, needed for contemporary dental practice.1 Traditionally, the curriculum in Australian and New Zealand dental schools has largely ignored the need for dentists to be educated in the field of sleep medicine, except for sleep bruxism. The education and training has been largely left to continuing education with little foundational oversight by organized dentistry or dental school accreditation standards within the context of the sleep medicine team.
The introduction and validation of oral appliances for the treatment of snoring and obstructive sleep apnea (OSA) has through years of research, resulted in dentists becoming involved in the treatment of patients with sleep disordered breathing (SDB).2,3 SDB is a group of common problems involving difficulties in breathing during sleep that may range from socially embarrassing snoring to severe and life-threatening OSA. These are caused primarily by negative pressures in the collapsible upper airway, which compromise the anatomic and physiologic capacity to maintain an adequate airway lumen during the various stages of sleep.4 SDB has been recognized to be a major risk factor for morbidity and mortality.5,6 There are cardiovascular, metabolic, and cognitive issues with undiagnosed and untreated OSA. Specifically, OSA has been linked to systemic hypertension, myocardial infarction, stroke, congestive heart failure, atrial fibrillation, carotid artery atherosclerosis, glucose intolerance, diabetes, depression, and excessive daytime sleepiness.7-9 Presence of any of these histories in the dental patient should precipitate questions about sleep disorders, even if the dentist is not involved in active treatments. Dentists can potentially treat OSA through growth and development orthodontic intervention in children,10 oral appliance therapy,11 or orthognathic surgery.12 Based upon the significant percentage of the population with OSA, ranging from 10% to 26% in Australian surveys,13 it is incumbent upon all health care providers to screen for these problems. Since dentists routinely examine the oral cavity, they also have a clear view of the oropharynx and are uniquely positioned to screen for potential anatomic risk features in patients with subjective or partner reports of SDB, unrestful sleep, or in patients reporting potentially associated medical problems. Therefore dentists could readily have an impact on the health status of our society if trained to a level of competency in sleep medicine.14 Screening as part of a wellness practice philosophy can evolve into active treatment by dentists subsequent to further training additional to a foundational dental school curriculum.
The American Academy of Sleep Medicine (AASM) practice parameters recommend that the “oral appliance should be fitted by qualified dental personnel who are trained and experienced in the overall care of oral health, the temporomandibular joint, dental occlusion, and associated oral structures. Dental management of patients with oral appliances should be overseen by practitioners who have undertaken serious training in sleep medicine and/or sleep related breathing disorders with focused emphasis on the proper protocol for diagnosis, treatment, and follow-up”.11 The Australian Dental Association (AuDA) has a policy statement on the “use of dental appliances to treat sleep disorders”.15 The AuDA has endorsed the guidelines of the AASM practice parameters for the use of oral appliances in the treatment of snoring and OSA.
The 2009 Australian Schedule of Dental Services and Glossary, which is the official AuDA document governing the item number for dentists to use when providing and invoicing oral appliance therapy to treat OSA,16 also makes reference to the AASM practice parameters.11 Similarly, the board of the Australasian Sleep Association (ASA) in July 2010 endorsed guidelines for the “use of dental appliance therapy for the treatment of SDB to ensure a minimum standard of clinical practice.”17 Again, this document has recommended the practice protocol of the AASM.11 In New Zealand, no formal guidelines exist on the use of oral appliances for snoring and OSA. Nevertheless, the New Zealand Dental Council (NZDC) consider the provision of “corrective dental appliances” to fall within the scope of dental practice.18 It is apparent that the Academies and Associations in Australia and New Zealand agree that dentists should be trained in the field of DSM if they choose to be involved in treating patients with SDB. However, all trainees should first be competent in conducting a routine sleep disorder history screening in a new patient as part of routine dental care.
Given the potential societal advantages of training the next generation of dentists in the field of DSM at Australian and New Zealand dental schools, the authors carried out an investigation of current predoctoral dental curriculum in both countries. The purpose was to establish the number of dental schools in Australia and New Zealand that include at least some DSM training at the predoctoral level and the current status of this education. Insight is anticipated for evolving structured and calibrated dental school sleep medicine education that will eventually become part of dental school accreditation standards and the foundation for standards of care in dental practice.
METHODS
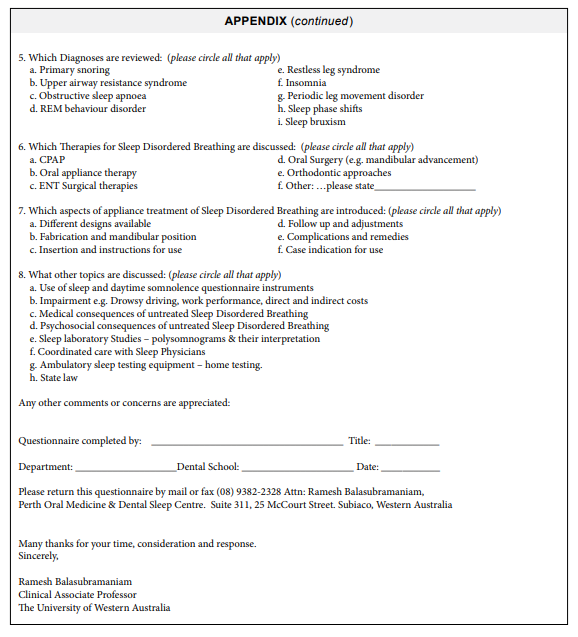
All 10 dental schools in Australia and New Zealand were sent a survey to gather information regarding their sleep medicine curriculum for the 2011 academic year. The battery of questions was based upon a study conducted on American dental schools.1 There were 8 categories in the questionnaire, which included: (1) hours spent teaching sleep medicine, (2) teaching methods, (3) department(s) involved in teaching, (4) topics discussed, (5) diagnosis reviewed, (6) all therapies discussed, (7) aspects of oral appliance therapy discussed, and (8) discussion of contemporary topics. (Appendix)
The questionnaires were mailed or e-mailed to the heads of all the dental schools in Australia and New Zealand who were instructed to forward it to the relevant course coordinator if necessary. The results were tabulated in Excel and analyzed.
RESULTS
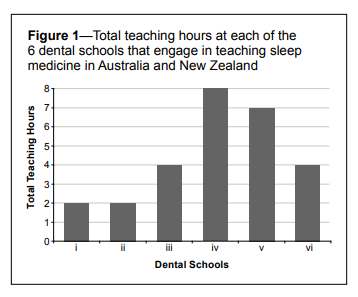
Nine of 10 dental schools responded to the survey. Three of the recently established dental schools were unable to complete the questionnaire, as their curriculum was underdeveloped and they had not yet graduated a class. The other 6 dental schools completed the survey, resulting in 85.7% response rate for schools that had graduated a class.The average total undergraduate teaching time was 4.5 h (SD 2.51) (range 2 to 8 h) among the 6 schools engaged in some teaching of sleep medicine in their curriculum. Figure 1 summarizes the range of predoctoral teaching time in sleep medicine at each of the Australian and New Zealand dental schools.
Figure 1Total teaching hours at each of the 6 dental schools that engage in teaching sleep medicine in Australia and New Zealand |
{kind=link}
It was apparent that 5 of the 6 dental schools spent most of their sleep medicine curriculum time teaching in the fifth year (of a 5-year course) with a mean of 2.5 h (SD 2.88); followed by the fourth and third years with a mean of 0.83 h (SD 0.75) each (Figure 2). Only 2 of the 6 dental schools spent time teaching sleep medicine in the second year with an average of 0.33 h (SD 0.51). Sleep medicine was not part of the curriculum in the first year of dental school in any of the reporting Universities.
Figure 2Distribution of total teaching hours in sleep medicine by dental school year throughout the 5 years of dental schooling |
{kind=link}
With regard to the learning experience of dental students, 55% of education time in sleep medicine was didactic, ranging from 1 hour to 4 hours. Two of the 6 dental schools had only a didactic component. One dental school had a 1-h hands-on (pre-clinical) laboratory component (4% of education time). Four of the 6 dental schools had a clinical component in their sleep medicine curriculum, which accounted for 41% of education time spent ranging from 0 to 5 hours. Detailed analysis revealed 2 of the 6 dental schools had a case-by-case and in-clinic discussion with 1 and 4 hours spent, respectively. Two of the dental schools had required rotation or clinical observation with 1 and 5 hours spent, respectively.
Two of the 6 dental schools teaching sleep medicine had multiple dental departments contributing to the undergraduate dental curriculum. In one dental school, the oral medicine and orofacial pain departments were co-involved in teaching sleep medicine. In the other dental school, the teaching was divided between the oral medicine, oral and maxillofacial surgery, and prosthodontic departments. The oral medicine specialty was the most commonly involved department teaching the sleep medicine curriculum (4 of the 6 dental schools). Of interest, all teaching was undertaken at the undergraduate level. None of the dental schools reported involvement in teaching sleep medicine at the postgraduate or dental specialty program level. There is no information in the survey about any curriculum coordination between departments.
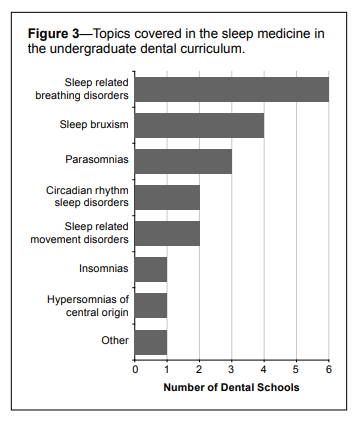
With regard to sleep medicine topics discussed, all 6 responding dental schools discussed SDB, and 67% of dental schools discussed sleep bruxism (SB). The other topics discussed are summarized in Figure 3. All 6 responding dental schools reviewed OSA as a diagnosis. A high percentage of dental schools reviewed the diagnosis of SB and primary snoring (83% and 67%, respectively). Fifty percent of dental schools reviewed the diagnosis of restless legs syndrome and upper airway resistance syndrome. Periodic limb movement disorder and insomnia were discussed by 33% and 17% of dental schools, respectively. Of note, the diagnosis of sleep phase shifts and REM behavior disorder were not discussed at all.
Figure 3Topics covered in the sleep medicine in the undergraduate dental curriculum. |
{kind=link}
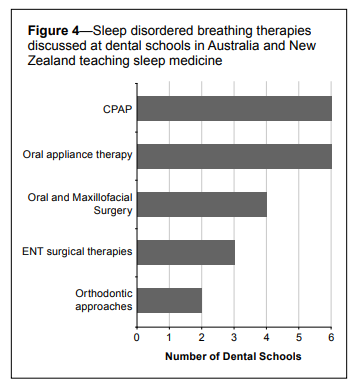
Dental school curriculum often involved discussion regarding various therapies for SDB (Figure 4). All dental schools involved in teaching sleep medicine covered the therapeutic interventions of continuous positive airway pressure (CPAP) and oral appliance therapy (OAT) in treating SDB. Four of the 6 responding dental schools discussed upper airway surgical therapies. Similarly, 4 responding dental schools discussed oral and maxillofacial surgical therapies (orthognathic surgery) for SDB. Most dental schools discussed various aspects of oral appliance therapy for SDB (Figure 5).
Figure 4Sleep disordered breathing therapies discussed at dental schools in Australia and New Zealand teaching sleep medicine |
{kind=link}
Figure 5Various aspects of oral appliance therapy for sleep disordered breathing discussed at dental schools teaching sleep medicine |
{kind=link}
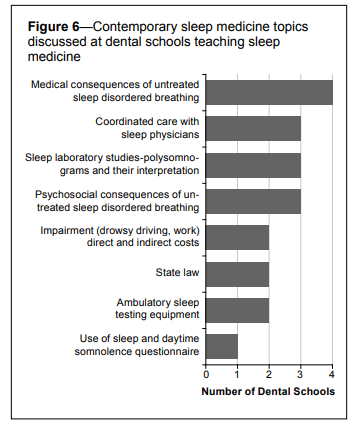
Figure 6 summarizes the percentage of the responding dental schools involved in discussion of contemporary topics in the field of sleep medicine. The medical consequences of untreated SDB were discussed by 67% of the responding dental schools teaching sleep medicine. Only 50% of the responding dental schools taught topics related to coordinated care with sleep physicians, diagnostic need and interpretation of sleep studies, and the psychological consequences of untreated SDB. This questions how much DSM is being taught within the concept of the sleep medicine team. Only 17% of the responding dental schools taught the use of screening questionnaires for use in catching occult or undiagnosed sleep disorders.
Figure 6Contemporary sleep medicine topics discussed at dental schools teaching sleep medicine |
{kind=link}
DISCUSSION
Six of the seven responding dental schools engaging in some teaching of sleep medicine in their curriculum (85.7%) averaged 4.5 total hours, ranging from 2 to 8 hours. This is comparable with the average time of 3.92 hours spent teaching this topic at United States (US) dental schools that taught sleep medicine. However, it should be noted that 24.5% of US dental schools responding reported they did not cover the topic of sleep medicine at all.1
Didactic education accounted for 55% of the time spent teaching sleep medicine. Conversely, the clinical component accounted for 41% of the education time in four dental schools, whereby time was spent either discussing cases or attending rotations or clinical observations (situation and responsibility undefined). Considering the overall low number of total hours, this suggests that sleep medicine, including sleep bruxism, does not have substantial pre-clinical foundation in the dental school curriculums, and likely does not go beyond an exposure-to competency. A preclinical hands-on experience was only reported by one school (4% of education time spent). Clinical experiences seem to have been mostly observational.
The current study found that most of the time spent teaching sleep medicine in dental schools (55%) was in the fifth year, which is typically a more clinically oriented year. One responding dental school taught the use of screening questionnaires, but it is not defined if any questions were being used in an oral diagnosis clinic in routine new patient intake. Sleep medicine was not offered as an elective in any of the dental schools surveyed. In their study of US dental schools, Simmons and Pullinger found didactic teaching made up 78.4% of time spent in sleep medicine and clinical teaching spent in sleep medicine was 35%.1 Overall, it appears the results of this Australia and New Zealand study were comparable to the current curriculum training experience of dental students in the US.
Sleep medicine education is no longer elective and definitely has a beginning presence in most Australian, New Zealand, and US dental schools, reflecting the scope of activities in contemporary dental practice, and probably individual faculty interest and expertise. However, the educational goals and competency standards aimed for in general dental programs, beyond exposure-to levels, needs discussion to evolve national education standards for a foundational curriculum and practice parameters on which to build post graduation, and to take into dental specialty training.
In the current study, the oral medicine department was most frequently involved in teaching the sleep medicine, often with additional departments involved, or perhaps teaching in parallel. This survey did not explore how individual departments coordinate and communicate with regard to topics covered or purpose. This was also a concern at US dental schools teaching sleep medicine.1
All the Australia and New Zealand dental schools mention or discuss SDB; however, surprisingly only 67% discussed sleep bruxism (SB), which remains the most managed sleep disorder in dentistry. Of interest, snoring, which is often a symptom of OSA, was discussed in only 67% of dental schools. A possible explanation could be preliminary nature of the education, whereby the details of differentiating symptomatic snoring from asymptomatic snoring was not discussed. Nevertheless, this is important to standards of care if dentistry becomes involved, to avoid practice of treating social snoring without a definitive sleep disorder diagnosis. In addition, more advanced sleep medicine topics were rarely or not at all discussed at the dental schools further, highlighting the superficial nature of the current education of sleep medicine at dental schools. More advanced sleep medicine topics are important if dentists are to become involved with medical colleagues in a sleep medicine team. While all dental schools discussed the two most common therapies for SDB, namely CPAP and OAT, other therapies including upper airway and oral and maxillofacial surgeries were not universally covered in the curriculum. Similar findings were noted at US dental schools.1
The field of DSM is a growing area of interest within dentistry. Dentists are being called upon by their medical colleagues to collaboratively treat patients with SDB. However, the question remains whether dentists have the foundational education required to competently treat patients with SDB. To date, there has been no formal study assessing educational preparedness of dentists in the field of sleep medicine in Australia and New Zealand. Bian in 2004 surveyed dentists in Indiana, USA, and found an overall deficiency in education regarding OSA and OAT.19 Undergraduate and postgraduate training were only reported by 16% and 30% of responders, respectively. Thirtytwo percent reportedly were self-taught. Of concern, 58% of responders were unable to identify common signs and symptoms of OSA, and 40% stated knowing little or nothing about OSA.
Mindell et al. studied sleep education in medical school curriculum across countries.20 Findings revealed only 6 of the 19 medical schools in Australia responded to the survey. It was noted that 369 minutes was spent teaching sleep medicine in Australian medical schools, which was higher than the average of 146 minutes spent in other medical schools sampled from various parts of the world. Regardless, this highlights the limited time spent teaching sleep medicine at medical schools in Australia, which is problematic if the dentist is expecting their patient’s physician to be knowledgeable These findings were consistent with other studies, underscoring deficiencies in sleep medicine education in medical schools in the United States.21,22 Of interest, training in nursing schools in sleep medicine in the US is also not established, but it has been recommended that 40 hours education be required, which raises the requirement bar considerably.23
The Australian Dental Council (ADC) is an independent body for dental education and training in Australia. It is an external accreditation authority for the Dental Board of Australia. It sets the standard required of newly qualified dentists to be considered “competent” to be able to care for the Australian public. Of concern, the ADC does not require competency in the field of DSM. In fact, this area of dentistry is not mentioned at all in the document on “Professional attributes and competencies of the newly qualified dentist”.24 Similarly, the NZDC and the New Zealand Dental Association do not address competency in the field of DSM.18 It is therefore not surprising that very little time is spent teaching sleep medicine at Australian and New Zealand dental schools. The administrators of dental schools could consider allocating more time teaching subjects such as DSM as part of foundational competencies. The current teaching of sleep medicine at dental schools might currently serve as a good introduction to the field but appears insufficient to safely treat patients with potentially associated serious medical conditions as required by the ASA and ADA guidelines.
The authors believe it is the responsibility of dental schools to provide foundational competencies in the field of DSM as required in all other aspects of dentistry. Universities should be the leaders in providing standards of care to reflect contemporary practice, and to protect patients. Competencies in DSM have been recommended by Simmons and Pullinger.1 All new graduates should be moderately competent and confident in new patient intake sleep history triage through portal questions. All new graduates should be able to conduct a more comprehensive sleep history in symptomatic patients and in patients with medical histories and comorbidities, which have associations with SDB. Comprehensive history can be augmented by self-scoring published sleep questionnaires, combined with clinical examination for oropharyngeal anatomic risk factors. Understanding the need and mechanism for referral for in lab polysomnography or out of sleep center test and motivating the patient to act requires an understanding and discussion of the potential medical consequences of untreated SDB. The dental graduate must be able to identify, refer, and document patients suspected of having SDB to their physician to request a sleep study and sleep diagnosis. Competency can only be achieved in these history and clinical screening requirements if they are routinely included in the Oral Diagnosis intake clinic process in dental schools for all patients, and the standard patient database. This is considered the first important step and is a requirement for all of dentistry and not limited to a DSM expert clinic. The next level involves more training and potential treatment based on understanding of the outcomes of the medical sleep test and report. If suggested by the sleep physician, the dental graduate must be able to assess for suitability for an oral appliance for patients with SDB, provided they have received further clinical training post-graduation to “qualified” status or make the referral to such qualified dentist. “Qualified” dentists would provide follow-up care and testing as recommended by the AASM practice parameters.11 Similar, recommendations have been made for training in the US1 ; however, as of this date, the American Dental Education Association and the Council on Dental Accreditation have yet to implement foundational standards for DSM training in the US. Meanwhile, implementation and the scope of a school’s DSM curriculum depend on the insight of each dental dean and the faculty, supported also by the input of recognized sleep medicine academies.
CONCLUSIONS
Dentists are uniquely positioned to help screen and co-treat SDB in a multidisciplinary approach, as part of a patients’ sleep medicine team. It is no longer a question of whether dentists can help identify undiagnosed and untreated SDB conditions, but rather how best to implement and participate in the field of sleep medicine. Currently there is an awareness level of education in most Australian and New Zealand dental schools; however, this falls short in foundational, screening, and treatment competencies. By working towards incorporating DSM education into dental school curriculum standards, dentists can improve quality of life, reduce the medical costs, protect patients, and create a greater awareness of the medical and social importance of good sleep.REFERENCES
2. Barnes M, McEvoy RD, Banks S, et al. Efficacy of positive airway pressure and oral appliance in mild to moderate obstructive sleep apnea. Am J Respir Crit Care Med 2004;170:656-64.
3. Gotsopoulos H, Chen C, Qian J, Cistulli PA. Oral appliance therapy improves symptoms in obstructive sleep apnea: a randomized, controlled trial. Am J Respir Crit Care Med 2002;166:743-8.
4. Sullivan CE, Issa FG. Obstructive sleep apnea. Clin Chest Med 1985;6:633- 50.
5. Marshall NS, Wong KK, Liu PY, Cullen SR, Knuiman MW, Grunstein RR. Sleep apnea as an independent risk factor for all-cause mortality: the Busselton Health Study. Sleep 2008;31:1079-85.
6. Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: eighteen-year follow-up of the Wisconsin sleep cohort. Sleep 2008;31:1071-8.
7. Marshall NS, Wong KK, Phillips CL, Liu PY, Knuiman MW, Grunstein RR. Is sleep apnea an independent risk factor for prevalent and incident diabetes in the Busselton Health Study J Clin Sleep Med 2009;5:15-20.
8. Pack AI. Advances in sleep-disordered breathing. Am J Respir Crit Care Med 2006;173:7-15.
9. Lee SA, Amis TC, Byth K, et al. Heavy snoring as a cause of carotid artery atherosclerosis. Sleep 2008;31:1207-13.
10. Villa MP, Rizzoli A, Miano S, Malagola C. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath 2011;15:179-84.
11. Kushida CA, Morgenthaler TI, Littner MR, et al. Practice parameters for the treatment of snoring and obstructive sleep apnea with oral appliances: an update for 2005. Sleep 2006;29:240-3.
12. Pirklbauer K, Russmueller G, Stiebellehner L, et al. Maxillomandibular advancement for treatment of obstructive sleep apnea syndrome: a systematic review. J Oral Maxillofac Surg 2011;69:e165-76.
13. Bearpark H, Elliott L, Grunstein R, et al. Snoring and sleep apnea. A population study in Australian men. Am J Respir Crit Care Med 1995;151:1459-65.
14. Ivanoff CS, Hottel TL, Pancratz F. Is there a place for teaching obstructive sleep apnea and snoring in the predoctoral dental curriculum? J Dent Educ 2012;76:1639-45.
15. Australian Dental Association Inc., Policy Statement 6.7: Use of dental appliances to treat sleep disorders. http://www.ada.org.au/about/policies. aspx. Accessed March 12, 2012.
16. The Australian Schedule of Dental Services and Glossary. 984: Bimaxillary oral appliance for diagnosed snoring and obstructive snoring and sleep apnoea. St Leonards: Australian Dental Association Inc., 2009.
17. Australasian Sleep Association: Dental appliance therapy for the treatment of sleep disordered breathing. http://www.sleep.org.au/about/ dental-orofacial. Accessed March 12, 2012.
18. New Zealand Dental Council: Health Practitioners Competence Assurance Act 2003, 2012:7.
19. Bian H. Knowledge, opinions, and clinical experience of general practice dentists toward obstructive sleep apnea and oral appliances. Sleep Breath 2004;8:85-90.
20. Mindell JA, Bartle A, Wahab NA, et al. Sleep education in medical school curriculum: a glimpse across countries. Sleep Med 2011;12:928-31.
21. Rosen RC, Rosekind M, Rosevear C, Cole WE, Dement WC. Physician education in sleep and sleep disorders: a national survey of U.S. medical schools. Sleep 1993;16:249-54.
22. Orr WC, Stahl ML, Dement WC, Reddington D. Physician education in sleep disorders. J Med Educ 1980;55:367-9.
23. Lee KA, Landis C, Chasens ER, et al. Sleep and chronobiology: recommendations for nursing education. Nurs Outlook 2004;52:126-33.
24. Australian Dental Council: Professional attributes and competencies of the newly qualified dentist. June 2010. http://http://www.adc.org.au/ documents/Attributes%20&%20Competencies_Dentist%20v1.0%20 Final%2010-06-11.pdf. Accessed March 12, 2012.
ACKNOWLEDGMENTS
The authors acknowledge Professor Marc Tennant and Associate Professor Estie Kruger of the Centre for Rural and Remote Oral Health for their assistance with this research.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May, 2013
Submitted in final revised form January, 2014
Accepted for publication January, 2014
Address correspondence to: Ramesh Balasubramaniam, Perth Oral Medicine & Dental Sleep Centre, St John of God Hospital, Subiaco Clinic, Suite 311, 25 McCourt Street, Subiaco, WA 6008, Australia; Tel: +618 9382 2325; Fax: +618 9382 2328; Email: ramesh.balasubramaniam@uwa.edu.au
DISCLOSURE STATEMENT
This was not an industry supported study. The protocol of this research project was approved by the Human Research Ethics Committee at the University of Western Australia. The authors have indicated no financial conflicts of interest. All authors have contributed significantly and are in agreement with the content of the manuscript.
APPENDIX
AppendixStudy on Sleep Disordered Breathing |
{kind=link}
Appendix (continued)Study on Sleep Disordered Breathing |
{kind=link}