Original Article 1, Issue 10.2
Crossover Sleep Testing as a Population Mousetrap for OSA
http://dx.doi.org/10.15331/jdsm.7288Michael S. Simmons, DMD, MSc, MPH, FAASM, FAAOP, Diplomate ABDSM, Diplomate ABOP1, Nina Haq, BS1, Jason Mostadim, BA1, Tatyana Franco, BA1, Dan I. Naim, MD2, Colin M. Shapiro, MBBCh, PhD, MRCPsych. FRCPC3
1 Encino Center for Sleep and TMJ Disorders; 2 Beverly Hills Lung and Sleep Institute, 3 University of Toronto, Canada, International Sleep Clinic - Parry Sound, Youthdale Child and Adolescent Sleep Clinic
ABSTRACT
Introduction:
Population-level obstructive sleep apnea (OSA) underdiagnosis is attributable in part to sleep testing challenges. Consumer interest has driven the rise of patient wearables as an easy alternative assessment of sleep. Newer home sleep apnea tests have crossover utility between patient wearable and medical grade information. This study assessed patient benefits of crossover sleep apnea testing (XSAT) in a dental clinic.
Methods:
A convenience sample of consecutive patients choosing XSAT (N=52) were assessed for sleep testing satisfaction in a retrospective observational study through a phone follow-up survey.
Results:
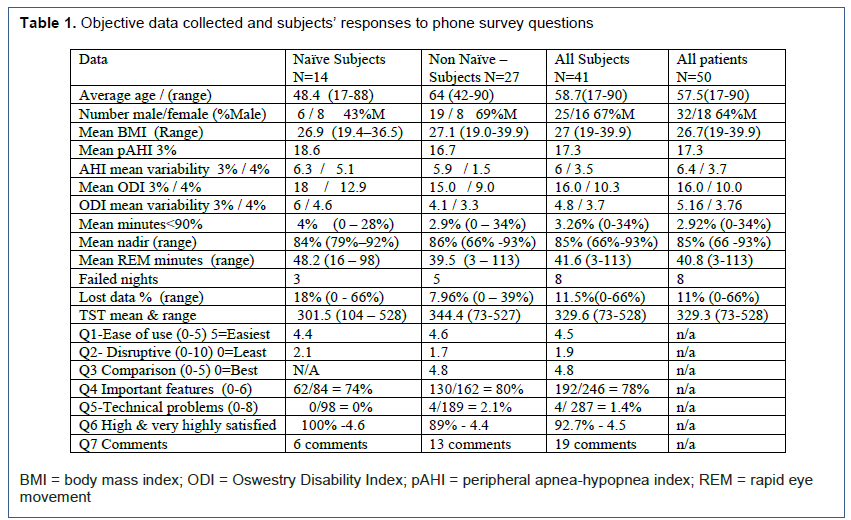
Two patients dropped out, and 41 completed the survey (82% response). Satisfaction with XSAT was high/very high in 93% of all survey-responders, and 100% of naïve (no past professional sleep test) survey-responders, with 1.2%experiencing technical problems. Failed test-nights occurred in 5.7% (8/141) test-nights with no failed studies. Average number of sleep-test nights were 2.8 (3.0 for naïve, 2.5 non-naïve). Twelve of 14 naïve survey-responders (six males, mean body mass index 26.9 kg/m2, mean age 48.4 years) had OSA (6 mild OSA). The night-to-night variability using 3% apnea-hypopnea criteria was 6.3 events/hr for naïve, 6.0 for all survey-responders, and 6.4 for all patients. XSAT benefit of “no need to return equipment” was important to 85% of non-naïve versus 64% of naïve survey-responders.
Conclusions:
XSAT is an early iteration paradigm shift in patient-friendly, professional sleep testing, potentially penetrating the market of undiagnosed OSA and addressing public health objectives.
Clinical Implication:
Increasing diagnosis of OSA can be achieved with friendly professional-level technology, enabling patient entry into sleep healthcare.
Keywords:
OSA; SRBD; HSAT; XSAT, Crossover sleep apnea testing; Gateway sleep testing: Night-to-Night variability: Multi-night testing: Public Health
Citation:
Simmons MS, Haq N, Mostadim J, Franco T, Naim DI, Shapiro CM. Crossover sleep testing as a population mousetrap for OSA. J Dent Sleep Med. 2023;10(2)
INTRODUCTION
Increasing the diagnosis of OSA remains a public health directive for sleep health, listed in both the Healthy People 2020 and 2030 health goals from the Office of Disease Prevention and Health Promotion of the US Department of Health and Human Services.1 OSA is a multifactorial disease related to breathing difficulties during sleep that falls under the classification of sleep- related breathing disorders (SRBD). On a worldwide basis, OSA prevalence is reported at 936 million individuals ages 30 to 69 years, of whom 55% have mild OSA.2 In the United States, prevalence for individuals age 30 to 69 years was reportedly greater than 54 million (33.2%), 2 of whom a very large proportion (93% of women, 82% of men) with moderate to severe symptomatic OSA remain undiagnosed. There is a greater undiagnosed proportion (98% of women, 90% of men) for mild to severe symptomatic OSA.3 One review from 20164 indicates 80% of those with OSA remain undiagnosed based on overly conservative OSA prevalence estimates of 12% of “adults”, whereas epidemiologic studies indicate at least a 26% OSA prevalence rate in the US. population ages 30 to 70 years.5 The prevalence of OSA continues to rise6,7 such that 49 of 193 countries evaluated had at least 50% of their population with OSA, and 48 of 193 countries had at least 25% of their population with moderate to severe OSA (apnea-hypopnea index [AHI] ≥15).2
Untreated OSA is associated with chronic health problems that include cardiovascular disease,8,9 metabolic disorders,10 cognitive impairment,11 memory loss,12 depression,13 and workplace and motor vehicle injuries and fatalities.14,15 Even mild OSA deserves treatment, according to the MERGE multicenter randomized controlled trial, where quality-of-life measures significantly improved in the mild OSA category with therapy for 3 months.16 The costs of untreated OSA are enormous,14, 17, 18 which when combined with the documented association of OSA with numerous adverse clinical outcomes, highlights the need for increased detection as the first step in the pathway to OSA management. One large case-control study of a nationally representative sample of the US Centers for Medicare & Medicaid Services (CMS) beneficiaries with OSA was found to have $20,000 / beneficiary in additional healthcare costs the year before OSA diagnosis as compared with matched control patients without OSA.19
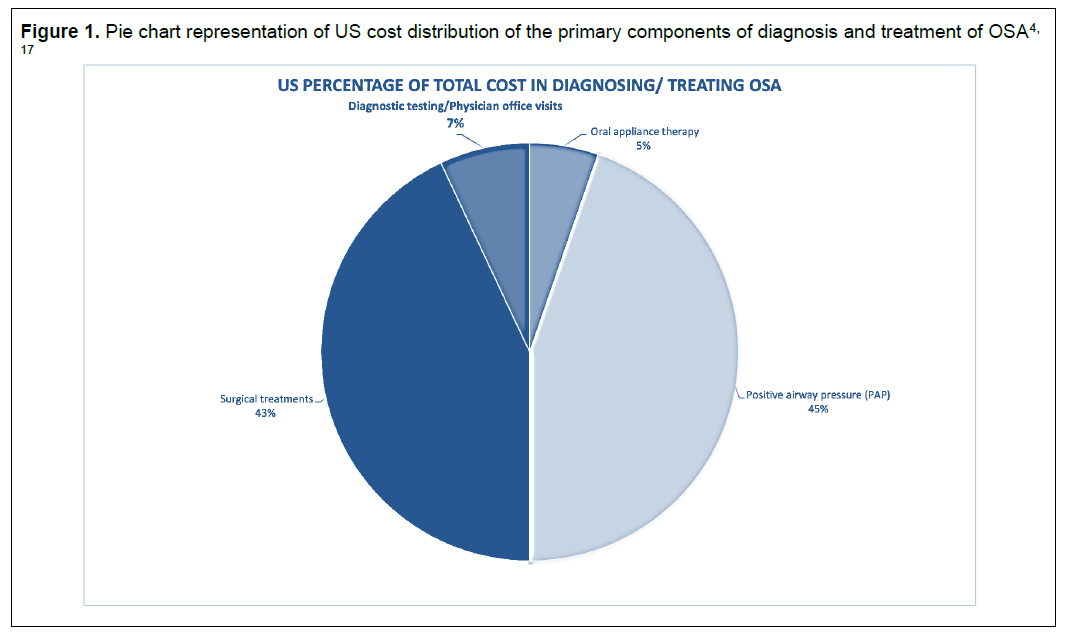
The reasons for OSA underdiagnosis include unawareness of the disease (both patients and their health care providers), lack of sufficient sleep health education;20,21 an inconvenient patient diagnostic process (e.g.., lack of readily available or agreed upon screening tools, limited access to sleep facilities and sleep specialists); limited hours of sleep testing; and high costs to diagnose and treat.2,22 In 2015, the estimated annual cost of diagnosing and treating OSA in the United States. was $12.4 billion (Figure 1) based on a 12% prevalence, with $50 billion needed to diagnose and treat every US adult with OSA, but with a projected savings of more than $100 billion from lost productivity, absenteeism, medical comorbidities, and motor vehicle and workplace injuries.23
Clearly, healthcare systems should seek strategies to raise awareness of OSA in order to diagnose and treat the condition to have a positive effect on population sleep health and healthcare expenditures. Diagnostic and delivery-of-care models may be developed so more patients can receive high-quality and efficient care, without the need for multiple office visits with sleep specialists, coupled with alternative payment models to accommodate more patients.24 For uncomplicated OSA (no significant health or sleep comorbidities), models of care without involvement of the very scarce and relatively dwindling number of sleep specialists,25,26 are only beginning to be developed that allow excellent clinical outcomes while potentially minimizing costs.27,28 In 2008, the CMS acceptance of home sleep apnea testing (HSAT) for OSA diagnosis streamlined the OSA diagnostic process and caused an abrupt paradigm shift from gold standard in-laboratory polysomnographic (labPSG) testing of sleep-related breathing disorder to include HSAT.29 At the same time, CMS also approved the innovative use of finger-based photoplethysmography (PPG) as an acceptable alternative surrogate data set to conventional airflow focused HSAT diagnostic data. HSAT devices were more patient friendly than labPSG sleep testing from a convenience, cost, availability, and access viewpoint, as well as facilitating sleep patterns to be reflected in the patient’s natural sleep environment for multinight testing.
The rationale for multinight and more hours of sleep testing is important as it relates to accommodating unsuccessful individual nights of sleep testing, often identified as sleep test failure rate. Failure in diagnosis may also be due to first night testing effects and night-to-night variability.30,31 Night-to-night variability may address different sleep architecture: between weekdays and weekends; altered work shift schedules; various levels of fatigue; different eating and exercise patterns; intermittent nasal rhinitis contributing to oral breathing; variable sleeping arrangements or body positions; and intermittent use of alcohol, tobacco, tetrahydrocannabinol, other recreational drugs or prescribed medications. Sleep variability may also be affected by the methods of substance intake such as vaping, inhaling, and smoking, which may cause transient inflammation of the upper airway structures. Alcohol consumption and/or smoking contributes to low oxygen saturation, respiratory depression, collapse of the oropharyngeal walls worsening severity of snoring and impaired sleep architecture especially in patients with OSA.32,33 In 2018, two-thirds of adults consumed alcoholic drinks, 5.1% heavy (>14 drinks/week for males, > 7 drinks/week for females), 15.5% moderate (4 to 14 drinks/week for males, 4 to 7 drinks/week for females) and 45.7% light drinkers (≤3 drinks/wk averaged over the year)34 with a subsequent 60.14% overall increase in alcohol consumption attributed to the COVID-19 effect.35 A cross-sectional study showed 35% of the patients who had OSA also smoked cigarettes, noting that smokers have a higher AHI than nonsmokers with an estimated 30.8 million adults (12.5%) who smoked in 2020.36
Another advantage to home-based multinight sleep testing is the patient can get feedback on the effects of best and worst sleep behaviors and gain insight into sleep health self-efficacy. The clearest understanding is that single-night testing in a strange environment represents an under-sampling of potential sleep related breathing pathophysiology, and no number of sensors can capture the needed information for best diagnosis with such limited time of sleep testing. For example, CMS approves labPSG OSA diagnosis in less than 2 hours of sleep testing with at least the number of events that would have been required in a 2-hour period (≥10 apnea/hypopnea events).37 Single-night HSAT may also be insufficient for accurate OSA diagnosis, and one study found 20% of patients were misdiagnosed with a single-night HSAT as having no or mild OSA when multinight testing revealed mild and moderate OSA, respectively.31 Another study of more than 47,000 patients found night-to-night fluctuations in the AHI using a HSAT, averaged 5.5 events/hour, resulting in over one-third of the patients having changes between diagnostic cut points.38 Even gold standard labPSGs have night-to-night variability and first -night effects typically resulting in a second night higher AHI. One labPSG 2-night study showed 55 of 125 (44%) more patients having an OSA diagnosis only in the second night.39 The first-night effects include decreases in: total sleep time (TST); sleep efficiency; rapid eye movement, along with increases in: sleep onset latency; wakefulness after sleep onset, and number of awakenings.
Recognizing public interest in sleep testing, direct to consumer offerings in wearable sleep trackers include wrist, ring and non-contact technology utilizing Bluetooth communication and smart phone apps which have grown to become commonplace. Sales in the wearable sleep tracker market grew at a compound annual growth rate of 6.5% between 2013 and 2021 and in 2021, the global market of the wearable sleep tracker accounted for approximately 4.5% of the overall wearable health device sales, amounting to approximately $1.9 billion in sales.40 Market growth for wearable sleep trackers is predicted to reach $4.2 billion in annual sales within the next 4 years.41 Many of these devices do not follow professional guidelines for HSAT testing, causing confusion and leading to “controversy about their application and validity.”42,23 Most of these devices collect unnecessary data that have no relevance when assessing sleep apnea. Although some of this “smart” technology44 purportedly provides heart rate, temperature, and movement and differentiates light, deep, and rapid eye movement sleep, many of these devices are advertised as “health” or “supplemental” equipment rather than HSAT devices to avoid Food and Drug Administration (FDA) scrutiny. Even so, there have been FDA warnings about limitations and accuracy of “over-the-counter” testing devices such as pulse oximeters due to lack of monitoring of safety and effectiveness.45
A new paradigm shift is now occurring for HSAT devices that are both professionally monitored using conventional sleep-related breathing disorder data and are comparable to patient-friendly tracking devices. One HSAT disposable OSA testing device is considered in this study as an XSAT, as it provides data from up to 100 hours of testing over approximately 3 years, individual patient ownership, limited contact with the patient’s anatomy, and remote monitoring of professional-level data for OSA diagnosis.46,47 XSAT may provide population-level sleep testing in the future. This may be especially helpful in underserved or remote areas. XSAT devices may also be positioned as gateway sleep testing for those unable to access sleep laboratories and sleep experts, for patients who have irregular and unpredictable sleep cycles, those with a large night-to-night variability in sleep, or those with difficulty falling asleep when attached to conventional sleep testing equipment. From a research perspective, an XSAT can be a great equalizer in independently assessing the effect of different medical interventions on OSA objective measures.48
This study evaluated patient satisfaction with an XSAT. It explores the benefits and shortfalls of this type of HSAT technology and addresses this new paradigm shift in diagnosing OSA that challenges current population-level gold standard testing with a more efficient, cost-effective, patient-friendly, and stepped care diagnostic process.
METHODS
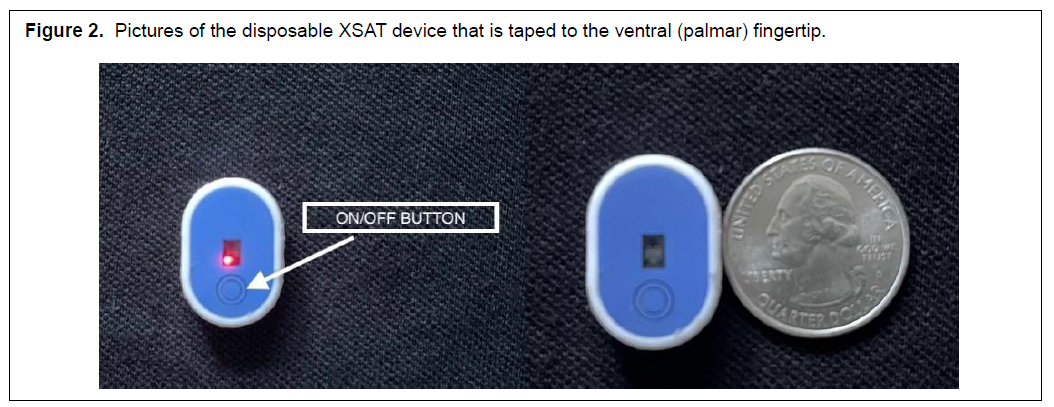
Consecutive patients with high probability of OSA, or those under current management for OSA, presenting to a single California-based dental office, were given (if indicated) the option to test their sleep using several HSAT devices. Patients who chose an overnight unattended sleep study utilizing the NightOwl XSAT were included in the study. This XSAT is a type IV HSAT device that contains a PPG sensor, pulse oximeter, and an accelerometer. The PPG sensor consists of two LEDs emitting red (660 nm) and infrared (880 nm) light, which is reflected from the peripheral tissue of the finger onto the photodiodes. The three-axis accelerometer picks up motion to provide an indication of activity/movement. Through its PPG sensor, this XSAT records pulsatile volume changes in the fingertip that reflect changes in sympathetic tone. In order to detect respiratory events, the proprietary software evaluates a decrease in peripheral arterial tone in combination with a drop in SpO2 oximetry, and an increase in heart rate. The resulting estimate of the AHI is referred to as the peripheral arterial tonometry estimated AHI or pAHI. Peripheral arterial tonometry (PAT)- based technology has a long history of validated use for the diagnosis of OSA and other health disorders and continues to be validated as an HSAT compared to labPSG.29 More specifically, this XSAT has been validated as an OSA testing instrument.46,47 In this study, patients who chose XSAT were given options as to the number of baseline nights of testing they would prefer.
A total of 52 XSAT devices were distributed to patients. The process for setup took less than 5 minutes by an assistant and included helping the patient download the NightOwl Companion app onto their mobile device, reviewing the position and tightness of finger probe placement with device adhesive tape, and confirming receipt of the device access code emailed to the patient. The patient was given an instruction page that outlined testing on multiple nights, including a variety of normal weekday and weekend nights and/or nights of alcohol, tobacco, recreational or other drug use as is typical for each individual. XSAT data, along with the patient’s comprehensive written medical/sleep history and clinical examination, were reviewed by the sleep physician (DN), who produced a diagnostic report consistent with current diagnostic standards. The sleep physician report was forwarded to the patient and their other healthcare provider(s).
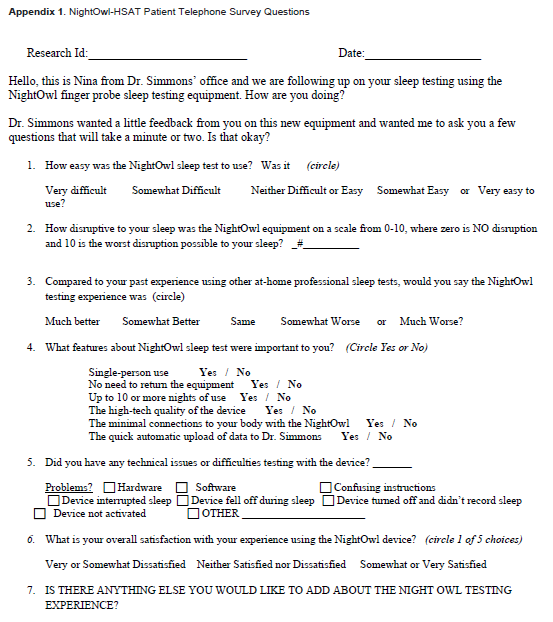
One or more phone calls were made to patients by a single research assistant (NH) for permission to ask XSAT follow-up phone survey questions, ranging from 1 week to 10 months after XSAT use. If permission was granted by the patient (now identified as subject or survey- responder)a 2- to 3-minute phone survey was completed. The phone survey followed a precise order with six quantitative followed by one qualitative question (Appendix 1). All subjects completed the phone survey. Subjective and objective data was collected and analyzed.
RESULTS
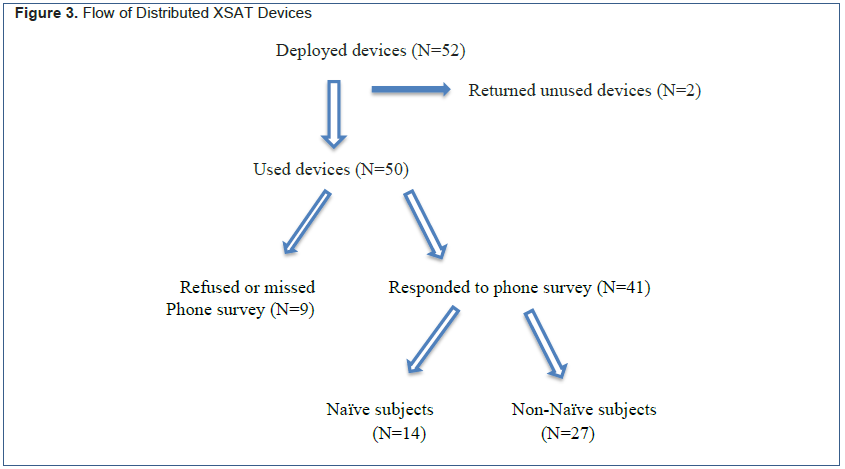
A total of 52 XSAT units were deployed, of which two were returned unused and were considered study dropouts. Of the 50 used XSAT devices, 41 subjects responded to the phone survey.
Data collected from all patients were tabulated (Table 1) and categorized into the following groups: “all subjects” who agreed to answer the phone survey; “naïve subjects” (defined as never having a professional sleep study before); “non-naïve subjects”; and “all patients”. There was an 82% response rate (41 of 50) for all patients, an 87.5% response rate (14 of 16) for the naïve patient group, and a 79.4% (27 of 34) response rate for non-naïve patient group.
Subjective Data
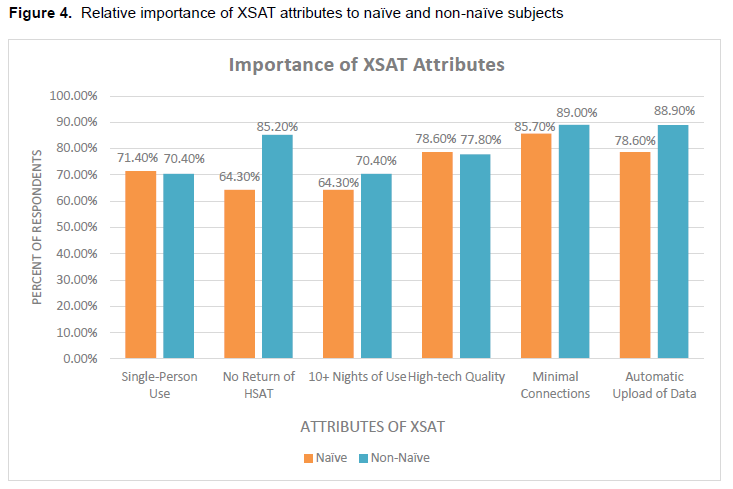
Subjects (N=41) divided into naïve (N=14) and non-nNaïve (N=27) groups (Figure 3) endorsed as “important“ up to six different attributes of the XSAT. Both the naïve and non-naïve subjects endorsed all survey-offered attributes of the XSAT, with a minimum of 60% of subjects finding all attributes important. Highly endorsed attributes, (defined as having more than 85% of subjects endorse as important), included only one attribute by both naïve and non-naïve subjects, namely the “minimal connections to your body“. Non-naïve subjects identified two other highly endorsed important attributes, including “no return of HSAT’ and “automatic upload of data.”
Non-naïve subjects endorsed as important “no need to return equipment“ 82.6% of the time versus 67% for Naïve subjects. Non-naïve subjects endorsed as important “automatic upload of data” 89% of the time verses 79% for naïve subjects.
Technical difficulties can contribute to failed test nights with any sleep test. Question #5 (Appendix 1) of the phone survey gave seven suggested reasons for technical difficulties that subjects may have had along with one (or more) optional added reason(s) to total 8 reasons. There were no endorsed technical difficulties reported by the naïve subjects (N=14) and a total of 4 out of a possible 216 (8x27) endorsed difficulties for the non-naïve group (N=27), making the total endorsed technical issues/difficulties as 1.2% (4 of 328). These difficulties were associated with hardware (2 of 41=4.9%), software (1 of 41=2.4%), and failure to record (1 of 41=2.4%). There were also six possible positive attributes subjects could endorse in the survey (Question 4, Appendix 1). Non-naïve in contrast to naïve subjects highly endorsed two important attributes of the XSAT-- “no return of HSAT’ and “automatic upload of data.” This probably reflects some past frustration with these components of other HSAT experiences and speaks to future approaches to improve repeat testing of OSA.
Historically, many patients report that their sleep test did not reflect their typical or problematic sleep cycle. It can be a hit-or-miss journey and for many a journey of frustration and invalidation. The ability to have feedback on whether the sleep cycle tested is reflective of the patient’s sleep problems is important but is not usually commented on within sleep test reports. This XSAT companion communication software automatically asks for this information from patients. Results indicated that the sleep cycle was highly representative about half the time (54%) and not representative 6% of the time (Figure 4). These data imply that 6% of sleep studies may miss the mark of catching the patient’s sleep complaint and another 40% may be somewhat representative. The advantage of multinight testing allows for 1 or more test nights to reflect representative sleep that the patient wants evaluated.
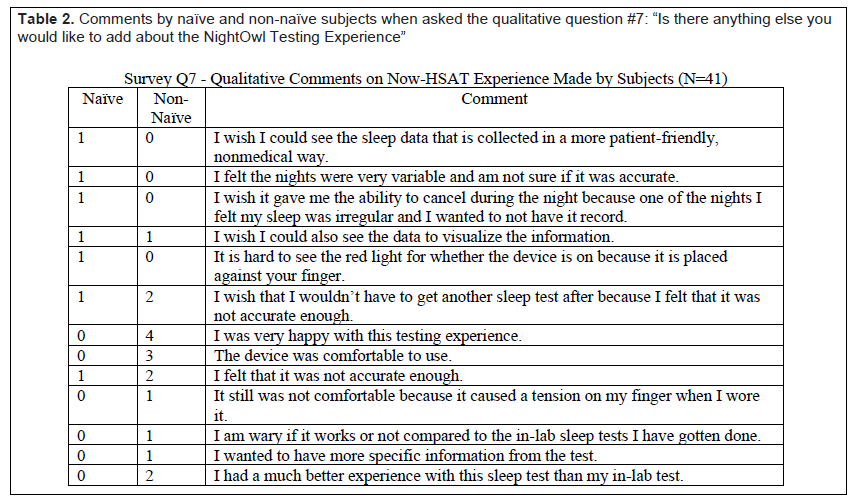
The one open-ended phone survey qualitative question (Question 7, Appendix 1), “Is there anything else you would like to add about the NightOwl testing experience”, received 7 comments from the Naïve subjects and 17 comments from the non-naïve subject group listed in Table 2.
Objective Data
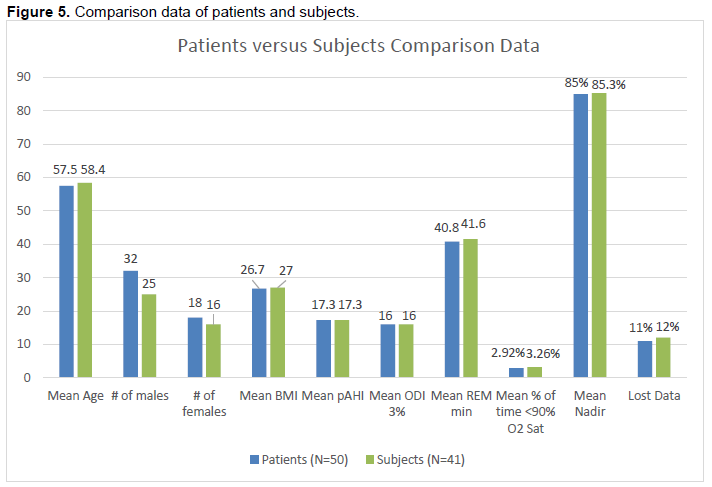
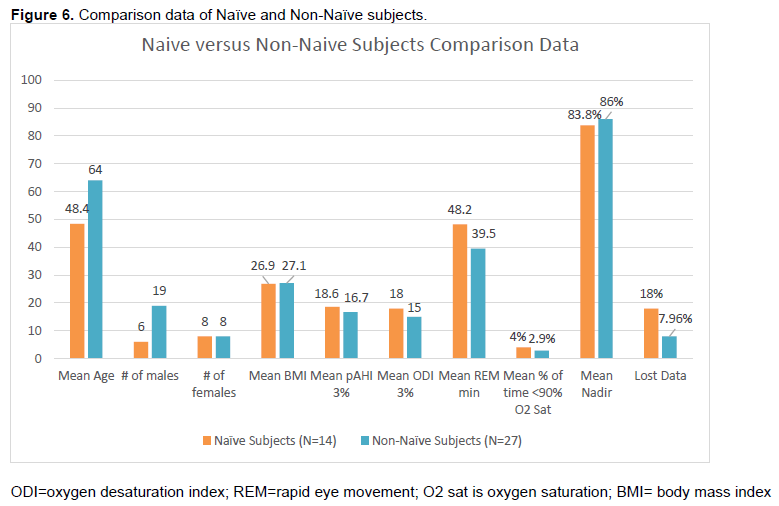
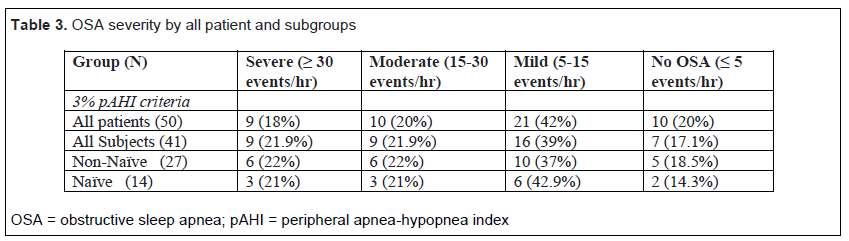
Classification of OSA severity in all patients using the 3% pAHI XSAT criteria indicated 80% (40 of 50) patients had remaining OSA (Table 3). Of those with OSA, there were 22.5% (9 of 40) with severe OSA, 25% (10 of 40) with moderate OSA, and 52.5% (21 of 40) with mild OSA criteria. The pAHI for 4% was evaluated for the 14 patients age 65 years or older. However, the software only automatically reported 4% pAHI starting in January 2022, so too few patients would have fit this category to report on their OSA severity using the CMS 4% criteria. Comparison data from the patients and subjects are shown in Figures 5 and 6.
Figure 1Pie chart representation of US cost distribution of the primary components of diagnosis and treatment of OSA |
{kind=link}
Figure 2Pictures of the disposable XSAT device that is taped to the ventral (palmar) fingertip |
{kind=link}
Figure 3Flow of Distributed XSAT Devices |
{kind=link}
Figure 4Relative importance of XSAT attributes to naïve and non-naïve subjects |
{kind=link}
Figure 5Comparison data of patients and subjects. |
{kind=link}
Figure 6Comparison data of Naïve |
{kind=link}
Table 1Objective data collected and subjects’ responses to phone survey questions |
{kind=link}
Table 2Comments by naïve and non-naïve subjects when asked the qualitative question #7: “Is there anything else you would like to add about the NightOwl Testing Experience” |
{kind=link}
Table 3OSA severity by all patient and subgroups |
{kind=link}
DISCUSSION
The 2030 Healthy People sleep directive SH-02 for OSA has the specific goal to “increase the proportion of adults (20+ years old) with sleep apnea symptoms who get evaluated by a health care provider”, listing a 37.1% target for this population to be evaluated.1 This represents a sizeable 30% increase from the 2020 Healthy People directive SH-01 target goal of 27.8% of “adults with symptoms of obstructive sleep apnea who seek medical evaluation.” By changing the “medical” evaluation” to one by a “health care provider” there is greater potential to achieve the directive goal. The goal is enabled by encouraging multiple pathways to diagnosis by others in addition to physicians, potentially including dentists, pharmacists, neuroscientists, and other primary healthcare providers. The engagement of nonphysicians in addressing OSA was previously encouraged by the 2006 landmark report titled “Sleep Disorders and Sleep Deprivation – An Unmet Public Health Problem” by the Institute of Medicine.49
This preliminary study of a dental clinic shows XSAT has high subject satisfaction, similar HSAT night failure rate at 5.7%, zero study failure rate, and applicability for diagnosing OSA. Because HSATs historically track total recorded time without specifically determining TST, there is a tendency to underreport apneas and hypopneas per hour of testing. This study showed that 88% (12 of 14) of the naïve patient group with a high probability for OSA had a diagnosis of OSA. This speaks to ease and frequency of diagnosis and when paired with a good patient experience can enable future studies once the streamlined process becomes known in the public sector. Naïve subjects had a diagnosis of mild OSA in 50% of studies, which is similar to large world population studies of OSA showing 55% have mild OSA.2 Night-to-night variability of the pAHI in this study addresses the effect of first-night effects as well as other night-to-night individual variability that may be attributed to many causes. The XSAT companion app allows up to 5 nights in one sleep study. There are several benefits to the multinight testing in addition to diagnosis of more OSA cases potentially missed in the first night. Some of these benefits include accommodating lost nights due to technical difficulties or specific patient challenges. Two patient (both subjects) challenges in this study accounted for 6 of the 8 failed nights. One patient had early dementia and the XSAT was managed by his spouse. He required all 5 nights for adequate testing and with this opportunity did not have a failed study. A second patient had severe sleep maintenance insomnia and required 5 test nights due to sleeping less than 2 hours at a time. The severe insomnia was associated with OSA and sleep data were acquired as a result of multiple nights testing. Moreover, the XSAT served as a gateway for the patient to have the confidence necessary to subsequently attend a split-night titration labPSG sleep study. This speaks to the necessity of a stepped care model of sleep testing because of the number of undiagnosed patients. It is likely that more labPSG’s will be required after penetration of crossover sleep testing is widely available.
The rationale for moving further away from gold standard labPSG testing as a first-line test for OSA is that labPSG is not designed specifically for OSA testing but rather to test a wide array of sleep disorders. Population-level testing for OSA requires population-level solutions, accessibility for general use, high efficiency, and cost effectiveness per test, which makes it both patient and clinician friendly. LabPSG is not optimally positioned for diagnosing the increasingly large number of patients with OSA.50 Because HSAT is the diagnostic procedure of choice by most patients with suspected OSA, the important question becomes which HSAT will have the most penetration into society to identify OSA at optimal sensitivity and specificity.51 Since the 2008 CMS approval of HSAT29 there has been a change in costs and utilization of sleep tests. Reports show CMS had a decreased annual expenditure for sleep tests, although the number performed increased by 9.1% since 2010.52 These same authors reported that in 2014, labPSG and HSAT accounted for 88% and 12%, respectively, of the almost one million total sleep studies as compared to year 2000, when HSAT studies numbered less than 1%. This change in use of HSAT represented a paradigm shift described as “the shot heard around the world” of sleep medicine.53 The market for HSAT devices subsequently exceeded $576.4 million in 2018 and this is expected to develop more than 14.4% in compound annual growth rate between 2019 and 2025.54 There has also been an increase seen in HSAT due to COVID-19 when in-laboratory sleep tests were dramatically reduced, resulting in lengthy wait time lists for labPSGs.55 An additional COVID-19 concern related to cross-contamination through HSAT use resulted in the availability of single-patient disposable testing devices, with the first FDA-approved disposable device released in February 2020.56 Disposable HSAT devices remove the patient’s financial responsibility for safekeeping of reusable medical equipment as well as eliminating time and effort spent in returning the device.
According to the American Academy of Sleep Medicine (AASM) labPSG remains the chosen sleep test for specific “complicated” patient groups, including patients with significant cardiorespiratory disease; potential respiratory muscle weakness due to neuromuscular conditions; awake hypoventilation or suspicion of sleep-related hypoventilation; chronic opioid medication use; history of stroke; or severe insomnia.57 In the AASM decision flowsheet of recommended sleep testing, labPSG is also suggested for symptoms of other significant sleep disorder(s), or environmental or personal factors that preclude the adequate acquisition and interpretation of data from a HSAT.57 LabPSG is also potentially important for central sleep apnea when an HSAT does not measure breathing effort, for some movement disorders of sleep and also for childhood sleep apnea. The AASM recommendations further indicate that HSAT should be reserved for diagnosis of uncomplicated adult patients presenting with signs and symptoms that indicate an increased risk of moderate to severe OSA, where increased risk is determined by the presence of excessive daytime sleepiness and at least two of the following three criteria: habitual loud snoring, witnessed apnea or gasping or choking, or diagnosed hypertension.57 This HSAT deployment criteria appears overly restrictive, as fewer than 20% of patients with OSA (15.5% male, 22.6% female) endorse excessive daytime sleepiness.58 In contrast, the CMS ruling CAG-00405N indicates that HSAT may be used to aid the diagnosis of OSA in all beneficiaries independent of OSA severity and whether or not they are “uncomplicated.”29 Although the 2017 AASM adult sleep testing recommendations,57 including preference of labPSG use, may be ideal at the individual patient level, this approach lacks penetration for population level diagnosis of OSA as evidenced by the continued enormous underdiagnosis of OSA.
There are many economic reasons to increase population-level diagnosis of OSA, with the estimated increased healthcare spending to treat undiagnosed OSA between $1,950 and $3,899 per patient per year as compared to patients without OSA,59 and there are also many other hidden costs.60 However, the cost comparison model for labPSG versus HSAT is complex due to the many variables, such as purpose of the study (e.g., diagnostic, baseline, titration, split-night), number of nights tested, HSAT device used, follow-up visits/telemedicine, failed study nights, and PSG laboratory space rental and equipment costs. One study reported a home-based management pathway for OSA diagnosis is less costly to the payer than a labPSG pathway whereas both pathways are similar in cost to the provider if delivering “high quality care.”61 It appears that per-night hard costs (sleep technician/overnight stay/testing equipment/disposable supply costs) for an XSAT are approximately 1% of the labPSG costs independent of follow-up care. This demonstrates a clear population cost advantage to support an XSAT tiered process for diagnosing OSA. As with other HSATs, there is a risk that other sleep disorders such as narcolepsy or sleep-related movement disorders (SRMD) would not be diagnosed with a XSAT. Although sleep-related movement disorders are determined by labPSG, the labPSG would not be diagnostic for narcolepsy without a subsequent multiple sleep latency test. A thorough sleep and medical history to assess the suspected sleep disorder is therefore important in deciding the correct sleep test to prescribe. The minimal cost of the XSAT is beneficial, currently at a population level, only to assess for OSA. Future professional-level crossover sleep testing may be focused on assessing other sleep disorders and sleep health behaviors.
Failed test nights may be differentiated from a failed sleep study. Failure study rates of the XSAT were considered to be zero due to the number of available testing nights, which accommodate one or more individual failed nights of sleep testing without overall sleep study failure. HSAT have been considered to have higher failure rates (5.3%) than labPSGs (3.1%) depending on the population tested.62 Lower failure rate may be due in part to the technician placing and correcting displaced sensors during the test. Contrary to some studies, HSAT failure rate may be similar to that of labPSG at 7.6%, depending on criteria for a successful study.63 Some authors have opined there is no “statistically robust set of parameters to characterize the performance of HSATs in general, and the agreement between HSATs and labPSG in particular.”64 Other authors pointed out the peril of reliance on correlation coefficients in comparing HSAT and labPSG as opposed to using diagnostic accuracy as a primary clinical performance endpoint.65 Finally, the importance of increased opportunity to identify OSA with multiple nights of HSAT is contrary to the strong recommendation from the AASM 2017 clinical practice guidelines that stipulate that if a single HSAT test is negative, inconclusive, or technically inadequate, labPSG should be performed for the diagnosis of OSA.57
When the Non-Naïve group (N=27) was asked to compare their past experience using other professional sleep testing to the XSAT crossover sleep test, using a 5-point Likert scale (ranging from much worse to much better), they scored the XSAT as a 4.8/5.0 better experience. This is an important finding that HSAT manufacturers will find of interest as it supports the paradigm shift in sleep testing alluded to in this study. Overall, a large percentage of Naïve and Non-Naïve subjects were “somewhat or very satisfied” with their experience using the XSAT, 100% for Naïve subjects, 87% for Non-Naïve subjects. These satisfaction percentages speak to the potential for more market penetration in professional sleep testing.
The role of the dentist in helping to identify more patients with undiagnosed OSA is increasing based on incidence and prevalence of OSA but must be done in a safe manner involving sleep physicians when possible and at a minimum, the patient’s treating physician(s). When medical or other sleep disorder comorbidities exist, the sleep physician becomes an integral team member and often team leader. With no medical or sleep comorbidities and mild to moderate OSA, the dentist can play an increasingly helpful role in reducing the burden of undiagnosed OSA by channeling patients into diagnosis through use of XSAT. This is important relative to the prevalence of OSA severity, in which according to one study of 400 adult subjects found 61% with mild OSA, 32% with moderate OSA, and 7% with severe OSA.66
Limitations to this study include a lack of confirmation of diagnostic accuracy using the XSAT, even though the outcome proportions are very similar to results found in much larger population studies2 and two studies have verified the accuracy of this specific XSAT.46,47 Different time delays between use of the XSAT and the phone survey completion existed and may affect the reliability of the answers. However, there was inherent variability in comparing this XSAT to previous experiences with other sleep testing by the various respondents over their historic testing timelines. The group itself could have bias in that they chose this XSAT versus other HSAT designs, which would lead to higher satisfaction ratings but also potentially dissatisfaction if it did not meet with their expectations. This study also compared measures of AHI, which may become an obsolete sleep metric because it is not a good reflection of cardiovascular health67-69 and future sleep crossover devices may place more emphasis on desaturation data. The closely guarded proprietary criteria used to define an apnea or hypopnea event with PPG sensor- based HSAT technology appear to be evolving as the sensor and interpretive software technology improves. Therefore, background changes in diagnostic algorithms may have occurred during this study without clinician end-user awareness, potentially affecting consistency of outcomes between patients. In this study, additional data showing both 3% pAHI and 4% pAHI were first provided automatically in 2022. The significance of using 3% or 4% criteria may complicate comparisons to labPSG data, as one large study of 500 patients having concomitant labPSG and PPG type HSAT (WatchPAT 200) testing found the HSAT device underreported by 6 events/hour using the 4% AHI criteria, but overreported prevalence by 4 events/hour using the 3% AHI criteria.70 Another study limitation is the lack of back-to-back satisfaction comparisons with other emerging professional quality multinight HSAT devices, including newer ring technology,71 contemporary larger footprint HSAT devices, and even comparisons to nonprofessional sleep tracking technology72 categorized by delivery platforms such as smart phones, wearable devices, and devices imbedded into the bed or fixtures in the sleep environment.73 This merits future research.
CONCLUSION
Sleep testing for OSA has both evolved and devolved. The evolution is the use of novel and more accurate testing devices; better algorithms that can interface with machine learning and artificial intelligence;74,75 machine-level consistency that avoids subjective interscorer variability; less cost per test night; increased accessibility; patient-friendly interfaces, and focus on the underserved. Sleep testing for OSA has devolved in that the number of hours of sleep within the confines of diagnostic testing is reduced, thereby realizing a smaller effect from intranight and internight variability that compromises accuracy. Periodic reassessment of sleep testing protocols due to technology, cost, and convenience had the last major overhaul in 2008 when CMS, at the request of the American Academy of Otolaryngology-Head and Neck Surgery, allowed for diagnosis of OSA by home sleep testing.29 At the same time, CMS approved novel technology that allowed plethysmography as an alternative and surrogate data source for the diagnosis of OSA, which continues to evolve.
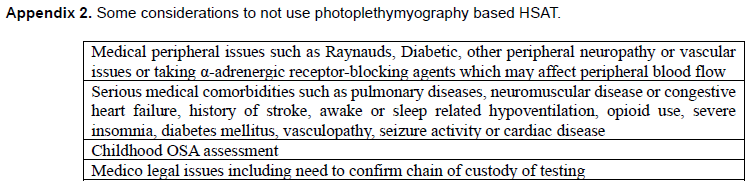
This XSAT represents the first widely available crossover sleep testing device at the professional level that fulfills many sleep testing advantages and can be considered the first iteration of a patient friendly, cloud-based, mass-produced solution to the lack of population-level diagnosis of OSA. There are still many areas of improvement needed, such as the ability to distinguish sleep architecture potentially resolved with add-on electroencephalographic technology76 or with newer HSAT technologies;71 addition of chain-of-custody information possibly using fingerprint identification technology; incorporation as needed of pulse rate variability information into the algorithm; addition of positional and snoring sound information; and the increased incorporation of artificial intelligence and machine learning into the diagnostic algorithm to improve diagnostic accuracy.77,78 Photoplethsmyography based sleep testing devices have current limitations in use (Appendix 2) and there are challenges to population-level deployment of this and other crossover technology as a better ‘mousetrap’ for the undiagnosed OSA, including incorporating XSAT technology in long-term maintenance testing of ongoing OSA therapies. The potential of this technology does not stop with addressing sleep disorders but can also contribute to sleep health education of patients through feedback loops, enabling sleep health self-efficacy. Other needed improvements in the software will include the flexibility to review raw data, explore more specific data of interest, and improved outcome reports that meet the interests of both patients and clinicians. Despite these limitations, which will undoubtably improve over time, this crossover technology represents the second paradigm shift and disruption in sleep testing in 5 decades. The opinion that “indiscriminate use of HSAT carries a risk of harm in the form of delayed diagnosis, mis-diagnosis, additional financial burden to the patient and health care system, and misallocation of limited diagnostic resources”75 marginalizes the logarithmically larger societal damage from missed diagnosis with current OSA testing standards that reach so few of the population.
Appendix 1NightOwl-HSAT Patient Telephone Survey Questions |
{kind=link}
Appendix 2Some considerations to not use photoplethymyography based HSAT. |
{kind=link}
CLINICAL IMPLICATIONS
In order to make drastic changes to the bottleneck of diagnosis of OSA, a more patient- and clinician-friendly, efficient, and cost-saving diagnostic process should be utilized in primary healthcare provider venues. Following a clearly outlined diagnostic protocol, many more providers will be able to diagnose and manage uncomplicated OSA, using a stepped care model whereby complicated cases can be swiftly referred to sleep specialists. This crossover technology may prove to be the answer to achieving significantly better population-based diagnosis of OSA, fulfilling and potentially exceeding Healthy People 2030 sleep health goals.
REFERENCES
https://health.gov/healthypeople/search?query=sleep+apnea https://www.healthypeople.gov/2020/topics-objectives/topic/sleep-health/objectives
Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698. doi: 10.1016/S2213-2600(19)30198-5. Epub 2019 Jul 9.
Young T, Evans L, Finn L, Palta M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women, Sleep. 1997; 20(9):705–706.
Frost & Sullivan, American Academy of Sleep Medicine. Hidden health crisis costing America billions: underdiagnosing and undertreating sleep apnea draining health care system. 2016. https://aasm.org/resources/pdf/sleep-apnea-economic-crisis.pdf
Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177(9):1006–1014.
Malhotra A, Orr JE, Owens RL. On the cutting edge of obstructive sleep apnoea: where next? Lancet Respir Med. 2015;3(5):397-403.
Osman AM, Carter SG, Carberry JC, Eckert DJ. Obstructive sleep apnea: current perspectives. Nat Sci Sleep. 2018;10:21-34. Published 2018 Jan 23. doi:10.2147/NSS.S124657
Kapur VK, Resnick HE, Gottlieb DJ, Sleep Heart Health Study Group Sleep disordered breathing and hypertension: does self-reported sleepiness modify the association? Sleep. 2008;31(8):1127–1132.
Walia HK, Li H, Rueschman M, et al. Association of severe obstructive sleep apnea and elevated blood pressure despite antihypertensive medication use. J Clin Sleep Med. 2014;10(8):835–843.
Drager LF, Togeiro SM, Polotsky VY, Lorenzi-Filho G. Obstructive sleep apnea: a cardiometabolic risk in obesity and the metabolic syndrome. J Am Coll Cardiol. 2013;62(7):569–576.
Olaithe M, Bucks RS, Hillman DR, Eastwood PR. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep Med Rev. 2018;38:39-49.
Romero E, Krakow B, Haynes P, Ulibarri V. Nocturia and snoring: predictive symptoms for obstructive sleep apnea. Sleep Breath. 2010;14(4):337–343.
Wheaton AG, Perry GS, Chapman DP, Croft JB. Sleep disordered breathing and depression among U.S. adults: National Health and Nutrition Examination Survey, 2005–2008. Sleep. 2012;35(4):461–467.
Mulgrew AT, Ryan CF, Fleetham JA, et al. The impact of obstructive sleep apnea and daytime sleepiness on work limitation. Sleep Med. 2007;9(1):42–53.
Howard ME, Desai AV, Grunstein RR, et al. Sleepiness, sleep-disordered breathing, and accident risk factors in commercial vehicle drivers. Am J Respir Crit Care Med. 2004;170(9):1014–1021.
Wimms AJ, Kelly JL, Turnbull CD, et al; MERGE trial investigators. Continuous positive airway pressure versus standard care for the treatment of people with mild obstructive sleep apnoea (MERGE): a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8(4):349-358.
Hillman DR, Murphy AS, Pezzullo L. The economic cost of sleep disorders. Sleep. 2006;29(3):299–305.
Sleep Health Foundation Asleep on the job: Costs of inadequate sleep in Australia. 2017:1–112. https://www.sleephealthfoundation.org.au/files/Asleep_on_the_job/Asleep_on_the_Job_SHF_report-WEB_small.pdf
Wickwire EM, Tom SE, Vadlamani A, et al. Older adult US Medicare beneficiaries with untreated obstructive sleep apnea are heavier users of health care than matched control patients. J Clin Sleep Med. 2020;16(1):81-89.
Mindell JA, Bartle A, Wahab NA, et al. Sleep education in medical school curriculum: a glimpse across countries. Sleep Med. 2011;12(9):928-931
Simmons MS, Pullinger A. Education in sleep disorders in US dental schools DDS programs. Sleep Breath. 2012;16(2):383-392.
Pendharkar SR, Povitz M, Bansback N, George C, Morrison D, Ayas NT; Canadian Sleep and Circadian Network. Testing and treatment for obstructive sleep apnea in Canada: funding models must change. CMAJ. 2017;189(49):E1524–E1528.
Watson NF. Health Care Savings: The economic value of diagnostic and therapeutic care for obstructive sleep apnea. J Clin Sleep Med 2016;12:1075–1077. [PubMed: 27448424]
Freedman N. Doing it better for less: Incorporating OSA management into alternative payment models. Chest. 2019 Jan;155(1):227-233.
Rosen IM. Report of the 2017 – 2018 AASM President Ilene M. Rosen June 5, 2017. Accessed March 3, 2023. https://aasm.org/resources/pdf/rosen-president-report-2017.pdf
Watson NF, Rosen IM, Chervin RD; Board of Directors of the American Academy of Sleep Medicine. The past is prologue: The future of sleep medicine. J Clin Sleep Med. 2017;13(1):127-135. Published 2017 Jan 15.
Antic NA, Buchan C, Esterman A, et al. A randomized controlled trial of nurse-led care for symptomatic moderate-severe obstructive sleep apnea. Am J Respir Crit Care Med. 2009;179(6):501-508.
Chai-Coetzer CL, Antic NA, Rowland LS, et al. Primary care vs specialist sleep center management of obstructive sleep apnea and daytime sleepiness and quality of life: a randomized trial. JAMA. 2013; 309: 997–1004.
Pub 100-03 Medicare National Coverage Determinations Centers for Medicare & Medicaid Services (CMS) Transmittal 86 2008 Determination. Department of Health and Human Services. July 3, 2008. Accessed March 3, 2023. cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R86NCD.pdf
Ahmadi N, Shapiro GK, Chung SA, Shapiro CM. Clinical diagnosis of sleep apnea based on single night of polysomnography vs. two nights of polysomnography. Sleep Breath. 2009;13(3):221–226.
Punjabi NM, Patil S, Crainiceanu C, Aurora RN. Variability and misclassification of sleep apnea severity based on multi-night testing. Chest. 2020;158(1):365-373.
Kolla BP, Foroughi M, Saeidifard F, Chakravorty S, Wang Z, Mansukhani MP. The impact of alcohol on breathing parameters during sleep: A systematic review and meta-analysis. Sleep Med Rev. 2018;42:59-67.
Memon J, Manganaro SN. Obstructive sleep-disordered breathing. [Updated 2021 Aug 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441909
Boersma P, Villarroel MA, Vahratian A. Heavy drinking among U.S. adults, 2018. NCHS Data Brief. 2020 Aug;(374):1-8. [35] Nationa Center for Drug Abuse Statistics- Alcohol abuse statistics https://drugabusestatistics.org/alcohol-abuse-statistics
Report 2020 on Current cigarette smoking among adults in the United States. Centers for Disease Conrol and Prevention. March 17, 2022. Accessed March 3, 2023. https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm#:~:text=In%202020%2C%20nearly%2013%20of,with%20a%20smoking-related%20disease.
Sleep Testing for Obstructive Sleep Apnea (OSA). Centers for Medicare and Medicaid. March 3, 2009. Accessed March 3, 2023. cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&NCAId=227&ver
CAG-00405N Decision Summary. Centers for Medicare and Medicaid. December 23, 2008. Accessed March 3, 2023. cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=Y&NCAId=227
Dzierzewski JM, Dautovich ND, Rybarczyk B, Taylor SA. Night-to-night fluctuations in sleep apnea severity: diagnostic and treatment implications. J Clin Sleep Med. 2020;16(4):539-544.
Skiba V, Goldstein C, Schotland H. Night-to-night variability in sleep disordered breathing and the utility of esophageal pressure monitoring in suspected obstructive sleep apnea. J Clin Sleep Med. 2015;11(6):597-602.
Wearable sleep trackers market. Future Marketing Insights. June 2022. Accessed March 3, 2023. www.futuremarketinsights.com/reports/wearable-sleep-trackers-market.
Arc Industry report on emerging trends. IndustryARC. Accessed March 3, 2023. industryarc.com/Report/19669/wearable-sleep-trackers-market.html
de Zambotti M, Cellini N, Goldstone A, Colrain IM, Baker FC. Wearable sleep technology in clinical and research settings. Med Sci Sports Exerc. 2019;51(7):1538-1557.
Al-Mardini M, Aloul F, Sagahyroon A, Al-Husseini L. Classifying obstructive sleep apnea using smartphones. J Biomed Inform. 2014;52:251-259.
Oura Ring homepage. Oura. Accessed March 3, 2023. ouraring.com/overview
FDA in brief: FDA warns about limitations and accuracy of pulse oximeters. Food and Drug Administratoin. February 19, 2021. Accessed March 3, 2023. fda.gov/news-events/fda-brief/fda-brief-fda-warns-about-limitations-and-accuracy-pulse-oximeters
Massie F, Mendes de Almeida D, Dreesen P, Thijs I, Vranken J, Klerkx S. An evaluation of the NightOwl home sleep apnea testing system. J Clin Sleep Med. 2018;14(10):1791–1796.
Van Pee B, Massie F, Vits S, et al. A multicentric validation study of a novel home sleep apnea test based on peripheral arterial tonometry. Sleep. 2022;Feb 2:zsac028.
Ni Y-N, Thomas RJ. A longitudinal study of the accuracy of positive airway pressure therapy machine-detected apnea-hypopnea events. J Clin Sleep Med. 2022;18(4):1121–1134.
Institute of Medicine (US) Committee on Sleep Medicine and Research. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. (Colten HR, Altevogt BM, eds. Washington (DC): National Academies Press; 2006 .http://www.ncbi.nlm.nih.gov/books/NBK19960/.
Safadi A, Etzioni T, Fliss D, Pillar G, Shapira C. The effect of the transition to home monitoring for the diagnosis of OSAS on test availability, waiting time, patient’s satisfaction, and outcome in a large health provider system. Sleep Disord. 2014;2014:418246.
Kuna ST, Gurubhagavatula I, Maislin G, et al. Noninferiority of functional outcome in ambulatory management of obstructive sleep apnoea. Am J Respir Crit Care Med. 2011;183:1238–1244.
Chiao W, Durr ML. Trends in sleep studies performed for Medicare beneficiaries. Laryngoscope. 2017;127(12):2891-2896.
Kryger M. Sleep medicine: the shot heard around the world. J Clin Sleep Med. 2012; 8(2):117-118.
Ugalmugle S, Swain R. Home sleep apnea testing devices market projections 2025. Global Market Insights Inc. Home Sleep Apnea Testing Devices Market Projections 2025 (gminsights.com) https://www.gminsights.com/industry-analysis/home-sleep-apnea-testing-devices-market
FDA clears new disposable home sleep apnea test. American Academy of Sleep Medicine. February 18, 2020. Accessed March 3, 2023. https://aasm.org/fda-clears-disposable-home-sleep-apnea-test/
Yoon, DW, Shin H-W. “Sleep Tests in the Non-Contact Era of the COVID-19 Pandemic: Home Sleep Tests Versus In-Laboratory Polysomnography.” Clin Exper Otorhinolaryngol 2020; 13(4):318-319. doi:10.21053/ceo.2020.01599
Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504.
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230-1235. doi: 10.1056/NEJM199304293281704. PMID: 8464434.
Knauert M, Naik S, Gillespie MB, Kryger M. Clinical consequences and economic costs of untreated obstructive sleep apnea syndrome. World J Otorhinolaryngol Head Neck Surg. 2015; 1(1):17-27. doi: 10.1016/j.wjorl.2015.08.001. PMID: 29204536; PMCID: PMC5698527.
Borsoi L, Armeni P, Donin G, Costa F, Ferini-Strambi L. The invisible costs of obstructive sleep apnea (OSA): Systematic review and cost-of-illness analysis. PLoS One. 2022; 17(5):e0268677. Doi: 10.1371/journal.pone.0268677. PMID: 35594257; PMCID: PMC9122203
Kim RD, Kapur VK, Redline-Bruch J, et al. An economic evaluation of home versus laboratory-based diagnosis of obstructive sleep apnea. Sleep. 2015;38(7):1027-1037. doi: 10.5665/sleep.4804. PMID: 26118558; PMCID:
Garg N, Rolle AJ, Lee TA, Prasad B. Home-based diagnosis of obstructive sleep apnea in an urban population. J Clin Sleep Med. 2014;10(8):879-885. doi: 10.5664/jcsm.3960. PMID: 25126034; PMCID: PMC4106942.
Alakuijala A, Tervamäki J, Maasilta P, Bachour A. Predicting technical success in home sleep apnea test. J Sleep Disor. 2019;8(1). doi:10.4172/2325-9639.1000226
Kirsch D. Autopilot and algorithms: accidents, errors, and the current need for human oversight. J Clin Sleep Med. 2020;16(10):1651–1652 .
Massie F, Van Pee B, Bergmann J. Correlations between home sleep apnea tests and polysomnography outcomes do not fully reflect the diagnostic accuracy of these tests. J Clin Sleep Med. 2022;18(3):871–876.
Arnadottir ES, Bjornsdottir E, Olafsdottir KA, Benediktsdottir B, Gislason T. Obstructive sleep apnoea in the general population: highly prevalent but minimal symptoms. Eur Respir J. 2016;47(1):194-202; DOI: 10.1183/13993003.01148[
Oldenburg O, Wellmann B, Buchholz A, et al. Nocturnal hypoxaemia is associated with increased mortality in stable heart failure patients. Eur Heart J. 2016;37(21):1695-1703. doi: 10.1093/eurheartj/ehv624. Epub 2015 Nov 26. PMID: 26612581.
Yasir M, Pervaiz A, Sankari A. Cardiovascular outcomes in sleep-disordered breathing: Are we under-estimating?. Front Neurol. 2022;13:801167. Published 2022 Mar 15. doi:10.3389/fneur.2022.801167
McEvoy RD, Antic NA, Heeley E, et al; SAVE Investigators and Coordinators. CPAP for prevention of cardiovascular events in Oobstructive Sleep Apnea. N Engl J Med. 2016 Sep 8;375(10):919-31. doi: 10.1056/NEJMoa1606599. Epub 2016 Aug 28. PMID: 27571048.
Ioachimescu OC, Allam JS, Samarghandi A, et al. Performance of peripheral arterial tonometry-based testing for the diagnosis of obstructive sleep apnea in a large sleep clinic cohort. J Clin Sleep Med. 2020;16(10):1663-1674. doi: 10.5664/jcsm.8620. PMID: 32515348; PMCID: PMC7954003.
Belun Ring Gu W, Leung L, Kwok KC, Wu I-C, Folz RJ, Chiang AA. Belun Ring Platform: a novel home sleep apnea testing system for assessment of obstructive sleep apnea. J Clin Sleep Med. 2020;16(9):1611–1617.
Robbins R, Seixas A, Masters LW, et al. Sleep tracking: A systematic review of the research using commercially available technology. Curr Sleep Med Rep. 2019;5(3):156-163. doi:10.1007/s40675-019-00150-1
Ko PR, Kientz JA, Choe EK, Kay M, Landis CA, Watson NF. Consumer sleep technologies: a review of the landscape. J Clin Sleep Me.d 2015;11(12):1455–1461.
Goldstein CA, Berry RB, Kent DT, et al.. Artificial intelligence in sleep medicine: an American Academy of Sleep Medicine position statement. J Clin Sleep Med. 2020;16(4):605–607. https://doi.org/10.5664/jcsm.8288
Stretch R, Ryden A, Fung CH, et al. Predicting nondiagnostic home sleep apnea tests using machine learning. J Clin Sleep Med. 2019;15(11):1599–1608.
da Silva Souto CF, Pätzold W, Wolf KI, et al. Flex-printed ear-EEG sensors for adequate sleep staging at home. Front Digit Health. 2021 Jun 30;3:688122. doi: 10.3389/fdgth.2021.688122. PMID: 34713159; PMCID: PMC8522006
Xu Y, Ou Q, Cheng Y, Lao M, Pei G. Comparative study of a wearable intelligent sleep monitor and polysomnography monitor for the diagnosis of obstructive sleep apnea. Sleep Breath. 2022 Mar 26. doi: 10.1007/s11325-022-02599-x. Epub ahead of print. PMID: 35347656.
Leppänen T, Varon C, de Zambotti M, Myllymaa S. Editorial: Machine learning and wearable technology in sleep medicine. Front Digit Health. 2022;4:845879. doi: 10.3389/fdgth.2022.845879. PMID: 35310551; PMCID: PMC8924044.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted April 11, 2022
Submitted in final revised form July 18, 2022
Accepted for publication October 15, 2022
Address correspondence to: Michael S. Simmons, DMD, MSc, MPH, Diplomate ABDSM, Diplomate ABOP; Director: Encino Center for Sleep and TMJ Disorders; Address: 16500 Ventura Blvd Suite 370., Encino CA, 91436 USA; Email: msimmons@g.ucla.edu