Original Article 1, Issue 10.1
Malocclusion in Pediatric Obstructive Sleep Apnea Referred for Sleep Study
http://dx.doi.org/10.15331/jdsm.7276Kazuma Kitagaito, DMD, MSD, MSE 1; Maida Lynn Chen, MD 2; Geoffrey M. Greenlee, DDS, MSD, MPH 1; Soleil Roberts, DMD, MSD 1; Anne-Marie Bollen, DDS, MS, PhD 1
1University of Washington, School of Dentistry, Department of Orthodontics, Seattle, Washington; 2University of Washington, School of Medicine, Department of Pediatrics, Pulmonary and Sleep Division, Seattle, Washington
ABSTRACT
Objectives/Introduction:
To assess the dentofacial characteristics in children referred to a tertiary pediatric sleep center.
Methods:
A prospective cross-sectional study was conducted among children (8 to 18 years old) who were undergoing evaluation at a pediatric sleep center. The data obtained included polysomnography results, profile photo, intraoral examination, and dental history questionnaire. Comparisons were made between groups based on severity of obstructive sleep apnea (OSA) (no, mild, or moderate-severe OSA), and separately by surgical status (surgically naïve vs postadenotonsillectomy).
Results:
A total of 95 patients enrolled in this study. Facial convexity of the moderate-severe OSA group showed a statistically significant difference (P=0.02) when compared to the no OSA group. Sixty-nine patients were in the surgically naïve group and 26 subjects were in the postadenotonsillectomy group. No statistically significant differences in dentofacial characteristics were found between the surgically naïve and postadenotonsillectomy groups.
Conclusions:
Facial convexity varied between the children in different OSA severity groups. There were no significant differences in the dentofacial characteristics between the children who had prior adenotonsillectomy and those who were surgically naïve. Although these findings are limited due to the small sample size and confounding variables, further study is warranted to better incorporate the role of dentofacial assessments and care in treatment.
Clinical Implications:
The presence or severity of pediatric OSA is not to be determined by dentofacial morphology alone, though there is a plausible role of quantifying dentofacial characteristics in advancing the care of those referred for OSA evaluation.
Keywords:
Pediatric OSA, Obstructive Sleep Apnea, Polysomnography, Adenotonsillectomy, PSG, Craniofacial Characteristics, Dentofacial Characteristics, Posterior Crossbite
Citation:
Kitagaito K, Chen ML, Greenlee GM, Roberts S, Bollen AM. Malocclusion in pediatric obstructive sleep apnea referred for sleep study. J Dent Sleep Med. 2023;10(1)
INTRODUCTION
Obstructive sleep apnea (OSA) is defined by a recurrent occlusion of the upper airway during sleep, resulting in gas exchange abnormalities and/or cortical arousals. In children, the sequelae of untreated OSA are associated with physical and psychosocial consequences on their development. The prevalence of childhood OSA is estimated to be between 1% to 4%.1
The American Academy of Pediatrics recommends adenotonsillectomy as the first-line treatment for pediatric OSA.2 Although severity of OSA may often improve, recent reports indicate the effectiveness of adenotonsillectomy to vary from 27.2% to 82.9%.3 At times adenotonsillectomy is performed in children suspected of having OSA even without definitive adenotonsillar hypertrophy. Lymphoid tissues may not be visibly hypertrophic during a standard physical examination when the child is awake; yet, it can still restrict a significant portion of the upper airway while the child is asleep.4 Nevertheless, adenotonsillectomy poses serious risks, such as airway hemorrhage and respiratory compromise resulting in oxygen desaturation and/or hypercapnia.5 Careful consideration should be made before surgical intervention is rendered, because the etiology of pediatric OSA is multifactorial.
There are several risk factors associated with pediatric OSA, including certain craniofacial and dentofacial characteristics that are of particular interest for the orthodontic community. These include a narrow maxilla, long facies, retrognathic mandibles, steeper mandibular plane angles, and tendency for class II malocclusion.6-11 Although some prior studies have not conclusively linked malocclusion to children younger than 10 years suspected of having OSA, the association is not well understood in older youth and adolescents, many of whom are in active community orthodontic care.12-14 Further evidence-based information, when coupled with clinical history, will better inform the clinician of the possibility of undiagnosed pediatric OSA. Therefore, referral to a sleep specialist may lead to possible early diagnosis via polysomnography and subsequent treatment.
Treatment for pediatric OSA has historically been adenotonsillectomy as the first line of treatment, but there has been growing interest and need for orthodontic intervention, particularly for patients who are not candidates for adenotonsillectomy or who have OSA refractory to adenotonsillectomy. A better understanding of the dentofacial features of these patients will help to shape the role of orthodontic treatment in the future, given the increasing recognition of adverse effects of untreated pediatric OSA.
OBJECTIVES
The purpose of this exploratory study was to evaluate the dentofacial characteristics (Angle classification, overjet, overbite, and facial profile) of children referred to a tertiary sleep center, and to stratify those features by severity of OSA and the surgical status (surgically naïve or postadenotonsillectomy).
MATERIALS AND METHODS
This was a prospectively recruited, cross-sectional sample of consecutive pediatric patients undergoing polysomnography (PSG) at an American Academy of Sleep Medicine (AASM) accredited tertiary pediatric sleep center. Patients met eligibility inclusion if they were between 8 to 18 years of age, and excluded if they had a documented congenital or acquired craniofacial syndrome, prior orthodontic treatment, or active participation in another research study on the night of PSG. Eligible patients were approached at the time of PSG, and written consent from guardians and assent from minors were obtained to participate in the study. This study was approved by the Institutional Review Board of the University of Washington.
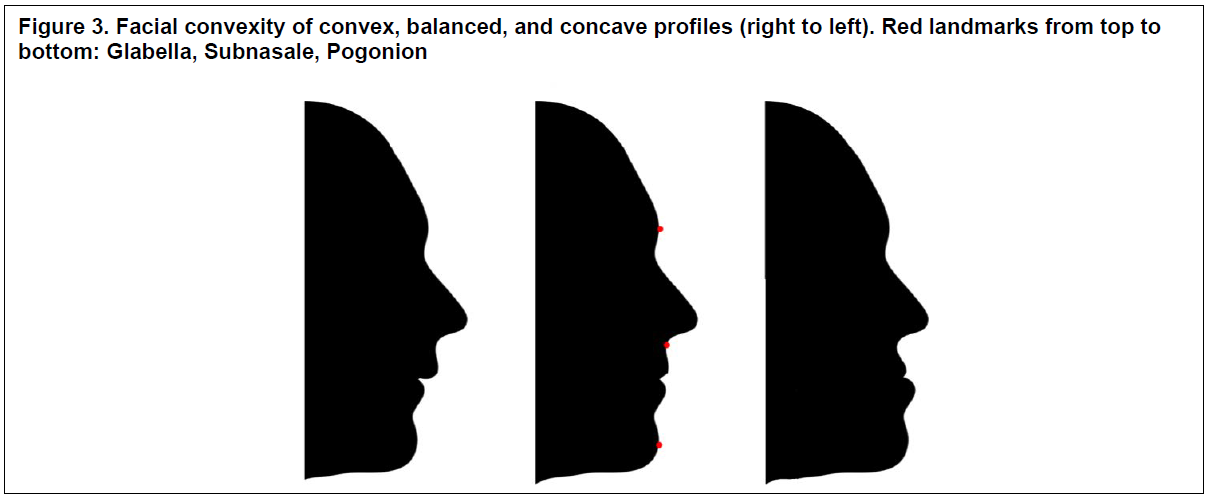
Data collected included a caregiver-completed demographic and dental history questionnaire, intraoral and extraoral examinations, and the PSG results. Surgical status of adenotonsillectomy was extracted from the medical record. Questionnaire items are shown in Supplemental Table 1. The extraoral and intraoral evaluations were done by the same investigator blinded to the results of the sleep study. Extraoral examination consisted of taking a profile photo to characterize facial convexity as balanced, convex, or concave using the patient’s glabella-subnasale-pogonion. Intraoral findings were recorded through clinical examination of each patient using a standardized examination form (Supplemental Table 2) with goals of quantifying overjet, overbite, and crossbite. PSG results were reviewed, and patients were stratified by severity of OSA based on obstructive apnea-hypopnea index (oAHI). The absence of OSA was defined by an oAHI < 1, mild OSA ≥ 1 to < 5, and moderate to severe OSA ≥5.15 Patient age, weight, height, and tonsil sizes by Brodsky score were also obtained from the PSG report.16 Age, weight, and height were used to calculate the patient’s body mass index (BMI) Z-score. Z-score of the BMI was used in lieu of BMI, as it predicts the level of obesity in the pediatric population using external reference, and it is standard in pediatric practice.17,18
STATISTICAL ANALYSIS
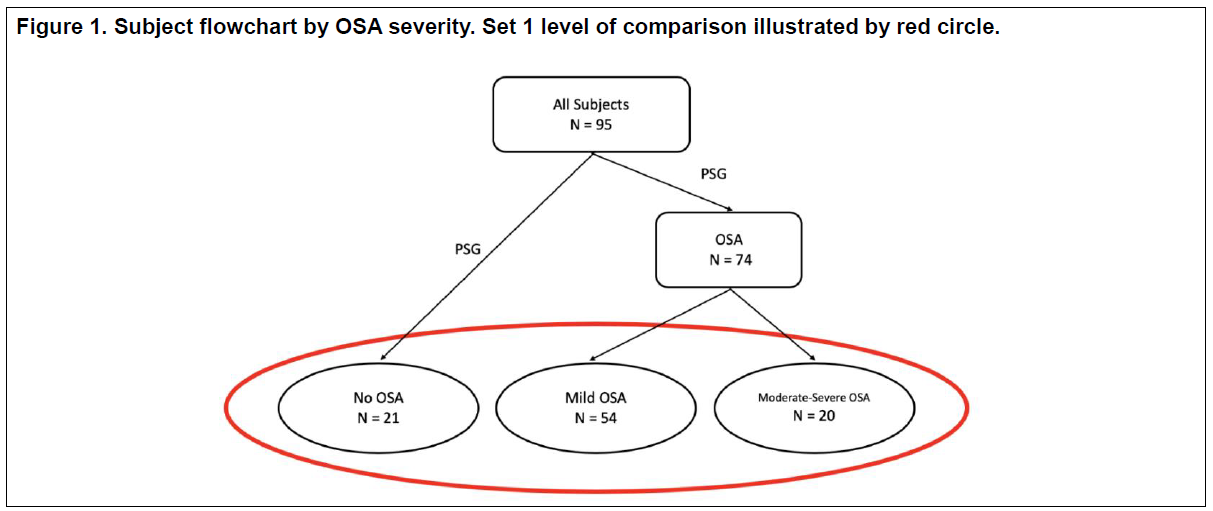
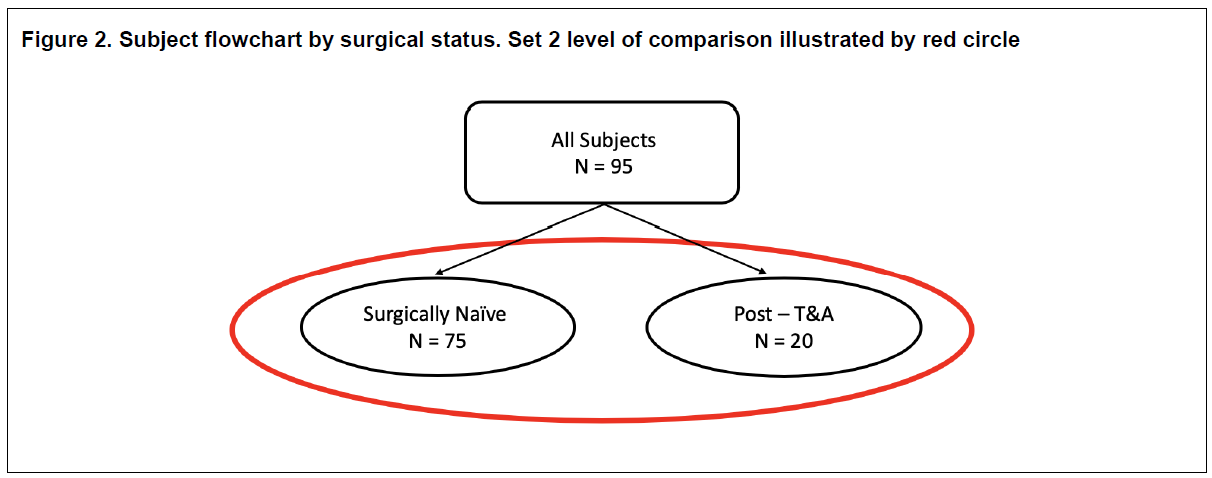
Descriptive statistics were used to illustrate patients’ baseline characteristics and questionnaire results; when pertinent, results were displayed as median with its interquartile range given asymmetric distribution. Two sets of categorical comparative analyses of dentofacial characteristics were performed: (1) between groups based on OSA severity (no, mild, and moderate-severe OSA), and (2) between groups based on surgical status (surgically naïve vs postadenotonsillectomy). Flowcharts are provided in Figures 1 and 2. Comparisons of dentofacial measurements (overjet, overbite, crossbite, and facial profile) in each set were done using Pearson chi-square or Fisher exact tests. Data were analyzed using Microsoft Excel software (version 16.54; Microsoft Corporation, Redmond, WA). Statistical significance was set at P <0.05.
RESULTS
A total of 97 consecutive patients were eligible for recruitment. Two patients declined to enroll in the study. The final enrollment was 95 subjects.
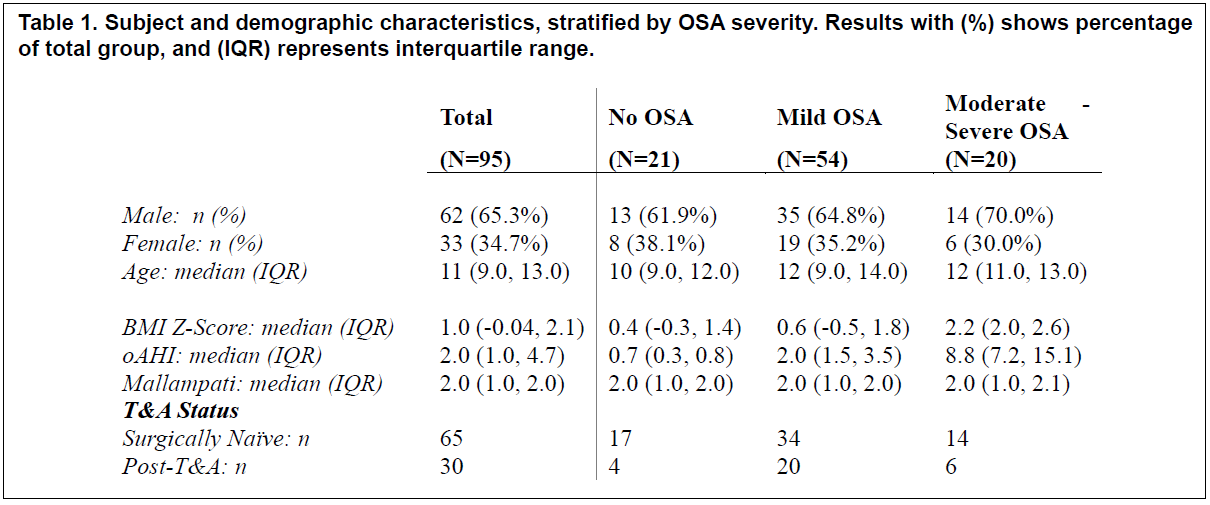
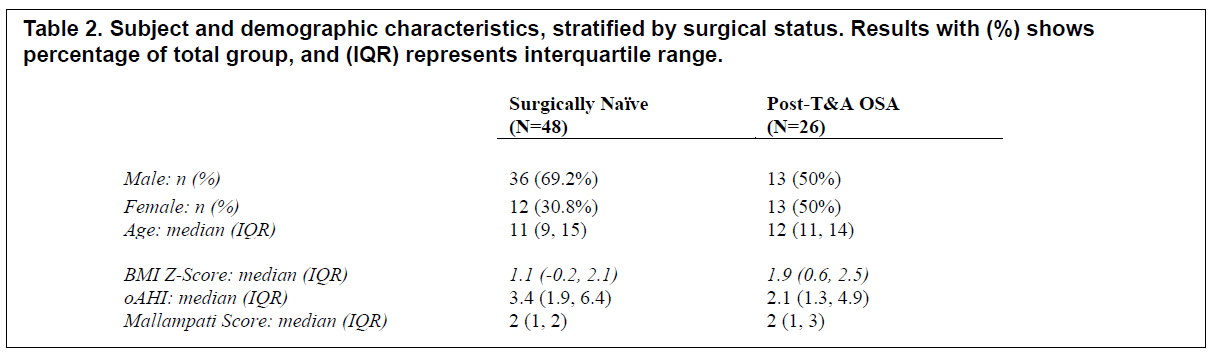
The median age of the subjects was 11 years old (interquartile range: 9.0 - 13.0). There were 62 males and 33 females in the sample. There was a similar distribution of males and females among all OSA groups. Demographic characteristics, stratified by OSA severity and surgical status, are presented in Table 1 and 2, respectively.
All 95 questionnaires were completed by the accompanying parent/guardian. Ninety-four patients reported going to the dental office for an examination in the past 6 months, and only one patient denied having a dental checkup in the past year.
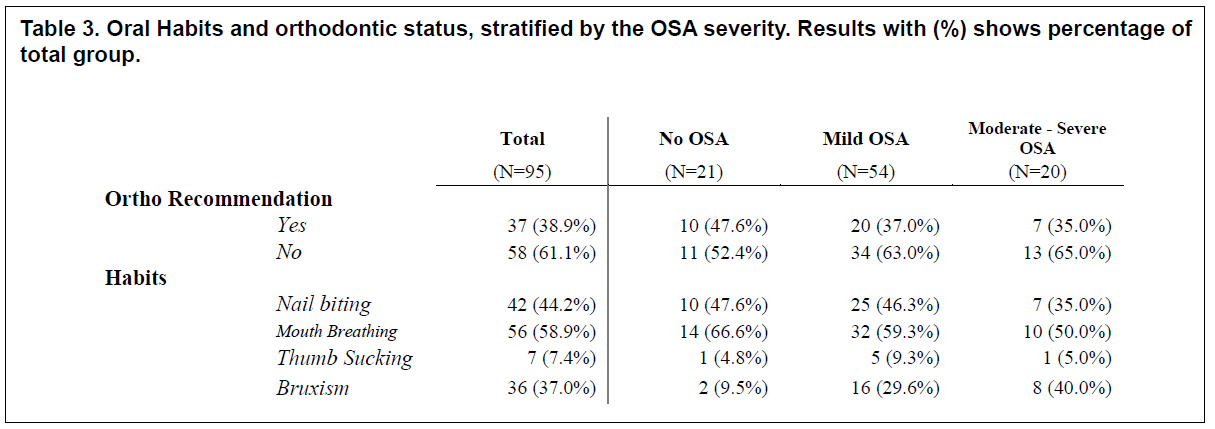
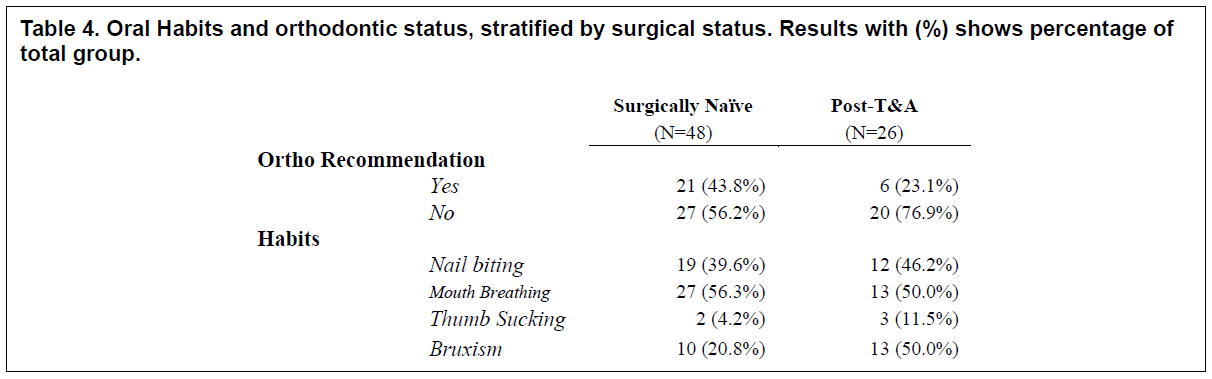
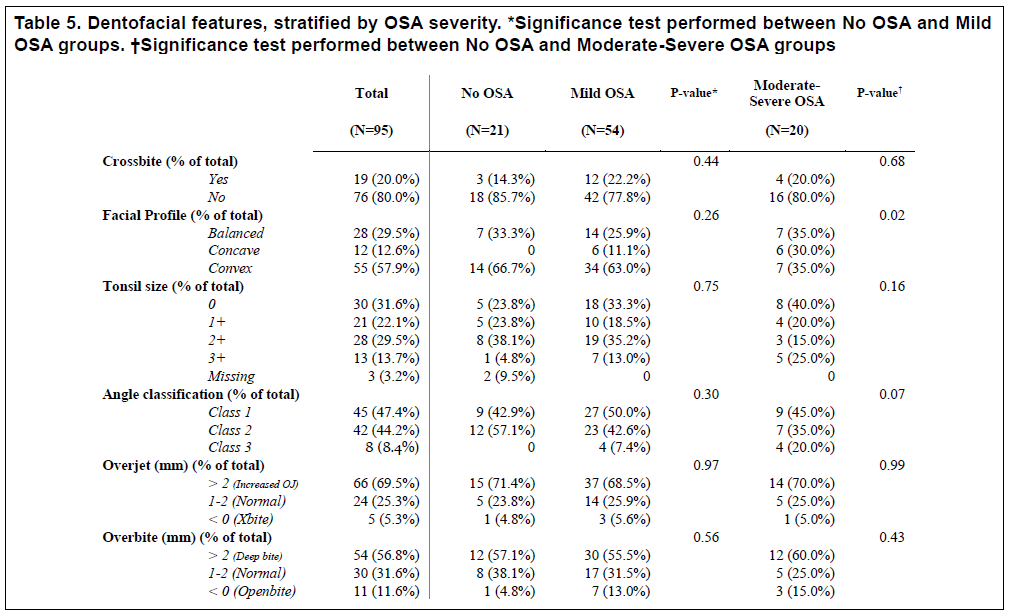
Rates of orthodontic treatment and oral habits history within the entire cohort, stratified by the OSA severity and surgical status, are presented in Table 3 and 4, respectively. Mouth breathing was the most common reported habit among all patients (59%). Orthodontic treatment had not been previously recommended in 61% of subjects. The oral examination findings for the complete cohort are presented in Table 5, and notable for most patients is the presence of convex facial profiles, with otherwise wide distributions of findings.
Set 1: Comparison by OSA Severity
Patients were stratified by OSA severity (no, mild, moderate-severe). Age and sex distributions were similar among OSA groups. However, median BMI Z-score was much higher in those with moderate-severe OSA, which was consistent with overweight and obesity in this population.15 Most patients had either mild or moderate-severe OSA on PSG, as expected given high pretest likelihood (referral bias). Of those with OSA, most were in the mild OSA group.
Oral habits were mostly not different between the severity groups with the exception of bruxism, which was markedly more common in those with moderate-severe OSA (40%) compared to the mild OSA group (30%), and also compared to the no OSA group (10%). Table 3 shows further distributions.
There was a statistically significant difference in the distribution of facial profile types (balanced, convex, and concave) of the moderate-severe OSA group when compared to the no OSA group (P=0.02). Facial profiles of the moderate-severe OSA group were evenly distributed among each profile. In comparison, most patients with a diagnosis of no OSA or mild OSA exhibited a greater prevalence of a convex facial profile. All the patients who exhibited a facial concavity had a diagnosis of some degree of OSA.
There were otherwise no differences between groups for presence or absence of crossbite, tonsil size, Angle classification, overjet, or overbite, as displayed in Table 5.
Set 2: Comparison by Surgical Status
Patients were stratified by surgical status (surgically naïve vs postadenotonsillectomy). Age, sex, and BMI distributions were not different between the groups. Furthermore, oAHI was not different between the groups.
Oral habits comparison was not different between the two surgical status groups. Table 4 shows further distributions.
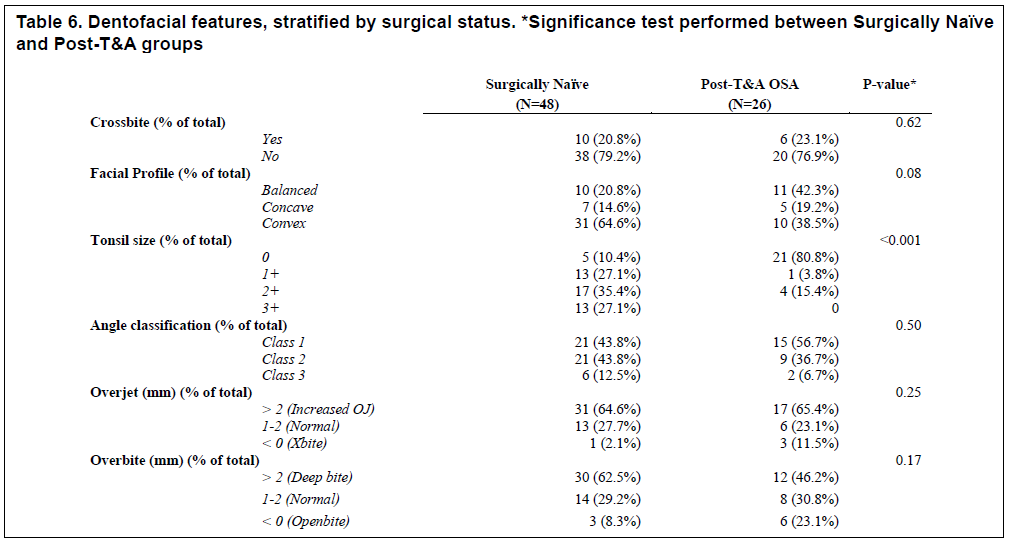
Overall, dentofacial characteristics did not largely vary between the two groups. As expected, the tonsil size was much smaller in the post adenotonsillectomy group compared to the surgically naïve group (P = <0.001).
There was a small trend of differences in the distribution of facial profiles between the postadenotonsillectomy group compared to the surgically naïve group (P = 0.08). Specifically, the surgically naïve group had 20.8% of patients with balanced/straight facial profile and 14.6% of patients with a concave facial profile. In comparison, the postadenotonsillectomy group had 42.3% of patients with balanced/straight facial profile and 19.2% of patients with a concave facial profile. Table 6 shows further distributions.
Figure 1Subject flowchart by OSA severity. Set 1 level of comparison illustrated by red circle. |
{kind=link}
Figure 2Subject flowchart by surgical status. Set 2 level of comparison illustrated by red circle. |
{kind=link}
Figure 3Facial convexity of convex, balanced, and concave profiles (right to left). Red landmarks from top to bottom: Glabella, Subnasale, Pogonion. |
{kind=link}
Table 1Subject and demographic characteristics, stratified by OSA severity. Results with (%) shows percentage of total group, and (IQR) represents interquartile range. (more ...) |
{kind=link}
Table 2Subject and demographic characteristics, stratified by surgical status. Results with (%) shows percentage of total group, and (IQR) represents interquartile range. (more ...) |
{kind=link}
Table 3Oral Habits and orthodontic status, stratified by the OSA severity. Results with (%) shows percentage of total group. |
{kind=link}
Table 4Oral Habits and orthodontic status, stratified by surgical status. Results with (%) shows percentage of total group. |
{kind=link}
Table 5Dentofacial features, stratified by OSA severity. *Significance test performed between No OSA and Mild OSA Groups. Significance test performed between No OSA and Moderate-Severe OSA groups. |
{kind=link}
Table 6Dentofacial features, stratified by surgical status. *Significance test performed between Surgically Naïve and Post-T&A groups. |
{kind=link}
DISCUSSION
The aim of this study was to characterize dentofacial characteristics (Angle classification, overjet, overbite, posterior crossbite, facial convexity) in children referred to a tertiary pediatric sleep center. Separate sets of comparisons were made between varying OSA severities (none, mild, moderate-severe OSA groups), and between groups based on surgical status (surgically naïve vs postadenotonsillectomy). These comparisons provide preliminary understanding of the relationships between dentofacial findings and prevalence of pediatric OSA in specific clinical scenarios. Multiple potential confounders and small sample size in this exploratory study precluded the ability to do further in-depth analysis on the relationships between dentofacial characteristics and certain subgroups, such as pediatric OSA refractory to adenotonsillectomy. Nevertheless, this study suggests that a fundamental difference may exist in facial profiles of children with a diagnosis of moderate to severe OSA. Given that this was ascertained by a simple facial photo, use of routine photos could prove to be a very simple, efficient, and noninvasive method to help better predict the likeliness of pediatric OSA. This could facilitate timely referral to a sleep specialist that would lead to earlier diagnosis via PSG and subsequent treatment.
This study provides some basic demographic characteristics of a tertiary pediatric sleep center, for which data are not common. Of this consecutive sample of otherwise healthy children referred for PSG, 77.9% of the patients had some level of OSA. This percentage is much higher than the reported prevalence of OSA in the general pediatric population, reflecting the significant referral bias still existent in the pediatric sleep field. Hence, this implies that many children with OSA are still undiagnosed and untreated. The ratio of males to females was 3 : 1, which was fairly consistent among all groups. In pediatric OSA, there is conflicting evidence when assessing for sex. 19.20 The study data indicate males having higher risk for pediatric OSA.
The study findings also confirm what other studies have reported, that those in whom moderate to severe OSA is diagnosed have much higher BMIs. Obesity is a well-known risk factor for pediatric OSA.21 Further, obesity is associated with other risk factors, such as poor nutritional health and higher prevalence of caries.22,23 The greater need for awareness and education of pediatric OSA in dental offices and pediatric practices, as well as support from pediatric nutritionists, is critical.
The facial profile of patients with moderate to severe OSA exhibited a tendency for facial concavity. All 12 patients with facial concavity had OSA, half of whom had mild OSA and the other half had moderate to severe OSA. The no OSA group did not have any patients with facial concavity. There are two possible reasons for this finding. First, there is a 2-year difference in median ages between the no OSA and moderate-severe OSA groups. That age gap may account for changes that occur during the adolescent growth spurt, driving the study findings. Second, BMIs were higher in the moderate-severe OSA group, which also may influence facial measurements. The relationship between facial profile, obesity, and OSA needs to be further studied. Although the study data did not have enough power to definitively conclude that facial concavity is associated with pediatric OSA, preliminary findings have physiologic plausibility to warrant pursuing future studies. Better control for obesity, as challenging it may be in pediatric OSA, will increase understanding.
There was no statistically significant difference in the presence of a posterior crossbite between the no OSA group and the mild OSA or moderate-severe OSA groups, despite reports that associate posterior crossbite with pediatric OSA.24 However, the no OSA group was a population referred for sleep- related breathing concerns, and hence may not be representative of the typical pediatric population. Interestingly, when comparing the percentage of crossbite in the entire study cohort to the percentages reported by the National Health and Nutrition Examination Survey (NHANES) III, the percentage of crossbite in the current study was far greater. The current study reported 20.0% of patients with crossbite in patients 8 to 18 years old, whereas NHANES III reported the percentage of 7.10% in patients 8 to 11 years old and 8.80% in patients 12 to 17 years old.25 Nevertheless, there were no differences in crossbite when comparing the different severities of OSA in the entire sample.
There have been numerous reports that mouth breathing is associated with anterior open bite.26,27 In the current study, 58.9% of the entire cohort reported mouth breathing. One-fourth of these patients did not have a diagnosis of clinical OSA, whereas most of the patients (57.1%) who reported mouth breathing had a diagnosis of mild OSA. Interestingly, slight tendency for decreased overbite was observed as the severity of OSA increased. This may be related to increasing rates of elevated BMI and facial concavity. Although it cannot be ascertained from research how mouth breathing contributes to pediatric OSA, the two are undoubtedly related and warrant further investigation.
There is evidence supporting association between class II malocclusion as measured by Angle classification and a diagnosis of pediatric OSA.28 In the current study, this association was not supported. The mild OSA and moderate-severe OSA groups did not exhibit statistically significant differences between the no OSA group in the Angle classification. In a previous study by Pirilä-Parkkinen et al., class II malocclusion was reported to be associated with increased overjet.29 In the current study, neither class II malocclusion nor overjet show any association with the different OSA groups. This difference may be explained by the variation in the age groups between the studies. In the study by Pirilä-Parkkinen et al., the median age of all patients is reported as 7.2 years. In the current study, the median age of all children was 11 years. It is a well-known phenomenon for class I occlusion to develop in children as they lose their primary dentition and allow for the permanent first molar to mesialize using the leeway space.30 Further investigation to assess the age, stage of dentition, and dental crowding or spacing of children will be beneficial to understand the relationship between class II malocclusion and pediatric OSA.
There was no statistical difference in the measured dentofacial characteristics between the surgically naïve group and postadenotonsillectomy group. The initial interest in understanding patients who underwent adenotonsillectomy was to evaluate if children who have undergone surgery have certain dentofacial features that were contributing to their residual OSA. By comparing the dentofacial characteristics of postadenotonsillectomy group to the features of the surgically naïve group, an attempt was made to uncover such qualities. The findings of the current study show that there was no difference between the two groups. Therefore, dentofacial characteristics alone cannot be considered a contributing factor for children with residual OSA.
There were several limitations of this study. First, given the exploratory nature of the study, the sample size of the patients in the moderate-severe OSA group was small (20) compared to the mild OSA patient group (54). However, even with this small sample size some suggestive findings about facial profiles were uncovered, supporting the need for appropriately powered studies in the future. Second, in set 2 comparing by surgical status, the patients in the surgically naïve group may contain patients who would undergo adenotonsillectomy in the future, after their initial sleep study. Moreover, because it could not be distinguished which patient will undergo adenotonsillectomy in the surgically naïve group, the two surgical status groups are not mutually exclusive. Thus, the comparison made between these two groups may not have exhibited significant differences. Nonetheless, results from the current study showed slight distribution differences in facial convexity. This illustrates a promising potential to further understand the relationship between facial convexity and OSA from dentofacial characteristic. Third, as mentioned previously, the no OSA group as control may not have been a true representation of the general pediatric population, given inherent concerns for sleep disordered breathing. However, these findings certainly are generalizable to the pediatric sleep field, which continues to see primarily the most symptomatic of all children. This limitation actually highlights the need for more OSA screening in both medicine and dentistry. Fourth, only a single assessor was used to analyze the facial convexity of the patients. Despite blinding to OSA diagnosis, the risk of systematic misclassification is increased with a single assessor.
In essence, this study supports a white paper published by the American Association of Orthodontics in 2019 that stated that “the presence of OSA cannot be determined by craniofacial morphology alone.”31 Though there are several pediatric sleep questionnaires that show promise as screening tools for children suspected to have OSA, none of these incorporate objective measures of dentofacial characteristics to combine both physical findings and reported signs and symptoms.32 The current study suggests that certain dentofacial characteristics may have the potential to be used as indicators to help dental professionals refer suspected pediatric OSA in addition to currently available OSA screens. Further research is beneficial to test the potential validity of these dentofacial indicators.
CONCLUSION
There was a statistically significant difference in the distribution of facial profile types when comparing between the no OSA and moderate-severe OSA groups. No significant differences in dentofacial characteristics were found between patients with different adenotonsillectomy surgical status. Limitations included small sample size and confounding factors such as obesity were present. Dentofacial characteristics alone cannot be used to determine the susceptibility nor severity of pediatric OSA.
ACKNOWLEDGMENTS
University of Washington, School of Dentistry, Department of Orthodontics
University of Washington Orthodontic Alumni Association
Seattle Children’s Hospital Sleep Medicine Program
REFERENCES
- Partinen M. Epidemiology of obstructive sleep apnea syndrome. Curr Opin Pulm Med. 1995;1(6):482-487.
- Schechter MS, Section on Pediatric Pulmonology, Subcommittee on Obstructive Sleep Apnea Syndrome. Technical report: diagnosis and management of childhood obstructive sleep apnea syndrome. Pediatrics. 2002;109(4):e69.
- Ahn YM. Treatment of obstructive sleep apnea in children. Korean J Pediatr. 2010;53(10):872-879.
- Garetz, SL. Adenotonsillectomy for obstructive sleep apnea in children. Wolters Kluwer/UpToDate. Available at: https://www.uptodate.com/contents/adenotonsillectomy-for-obstructive-sleep-apnea-in-children. Accessed: November 13, 2020
- McColley SA, April MM, Carroll JL, Naclerio RM, Loughlin GM. Respiratory compromise after adenotonsillectomy in children with obstructive sleep apnea. Arch Otolaryngol Head Neck Surg. 1992;118(9):940–943. doi:10.1001/archotol.1992.01880090056017
- Agren K, Nordlander B, Linder-Aronsson S, Zettergren-Wijk L, Svanborg E. Children with nocturnal upper airway obstruction: postoperative orthodontic and respiratory improvement. Acta Otolaryngol.1998;118 :581– 587.
- Zucconi M, Caprioglio A, Calori G, et al. Craniofacial modifications in children with habitual snoring and obstructive sleep apnoea: a case-control study. Eur Respir J. 1999;13(2):411-417.
- Flores-Mir C, Korayem M, Heo G, Witmans M, Major MP, Major PW. Craniofacial morphological characteristics in children with obstructive sleep apnea syndrome: a systematic review and meta-analysis. J Am Dent Assoc. 2013;144(3):269-277.
- Huynh NT. Morton PD, Rompré PH, Papadakis A, Remise C. Associations between sleep-disordered breathing symptoms and facial and dental morphometry, assessed with screening examinations. Am J Orthod Dentofac Orthop. 2011;140(6): 762 – 770.
- Souki BQ, Lopes PB, Pereira TB, Franco LP, Becker HM, Oliveira DD. Mouth breathing children and cephalometric pattern: does the stage of dental development matter?. Int J Pediatr Otorhinolaryngol. 2012;76(6):837-41.
- Mahony D, Karsten A, Linder-Aronson S. Effects of adenoidectomy and changed mode of breathing on incisor and molar dentoalveolar heights and anterior face heights. Aust Orthod J. 2004;20(2):93-98.
- Pliska BT, Lee J, Chadha, N. Prevalence of malocclusion in children with sleep-disordered breathing. J Dent Sleep Med. 2017;4(2):41-44.
- Galeotti A, Festa P, Viarani V, et al. Prevalence of malocclusion in children with obstructive sleep apnoea. Orthod Craniofac Res. 2018;21(4):242-247.
- Cohen-Levy J, Quintal MC, Rompré P, Almeida F, Huynh N. Prevalence of malocclusions and oral dysfunctions in children with persistent sleep-disordered breathing after adenotonsillectomy in the long term. J Clin Sleep Med. 2020;16(8):1357-1368.
- Marcus CL, Moore RH, Rosen CL, et al; Childhood Adenotonsillectomy Trial (CHAT). A randomized trial of adenotonsillectomy for childhood sleep apnea. N Engl J Med. 2013;368(25):2366-2376. doi: 10.1056/NEJMoa1215881. Epub 2013 May 21. PMID: 23692173; PMCID: PMC3756808.
- Brodsky L. Modern assessment of tonsils and adenoids. Pediatr Clin North Am. 1989;36(6):1551-1569. doi: 10.1016/s0031-3955(16)36806-7. PMID: 2685730.
- Must A, Anderson S. Body mass index in children and adolescents: considerations for population-based applications. Int J Obes. 2006;30:590–594.
- Centers for Disease Control and Prevention. (2002). 2000 CDC Growth Charts for the United States: Methods and Development. Atlanta, GA: US Department of Health and Human Services. Retrieved from https://www.cdc.gov/nchs/data/series/sr_11/sr11_246.pdf
- Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea. Proc Am Thorac Soc. 2008;5(2):242-252.
- Brockmann PE, Koren D, Kheirandish-Gozal L, Gozal D. Gender dimorphism in pediatric OSA: Is it for real?. Respir Physiol Neurobiol. 2017;245:83-88.
- Marcus CL, Greene MG, Carroll JL. Blood pressure in children with obstructive sleep apnea. Am J Respir Crit Care Med. 1998;157(4 Pt 1):1098-1103.
- Marshall TA, Eichenberger-Gilmore JM, Broffitt BA, Warren JJ, Levy, S.M. (2007), Dental caries and childhood obesity: roles of diet and socioeconomic status. Community Dent Oral Epidemiol. 2007;35: 449-458.
- Elger W, Kiess W, Körner A, Schrock A, Vogel M, Hirsch C. Influence of overweight/obesity, socioeconomic status, and oral hygiene on caries in primary dentition. J Investig Clin Dent. 2019 May;10(2):e12394. doi: 10.1111/jicd.12394. Epub 2019 Jan 20. PMID: 30663274.
- Carvalho FR, Lentini-Oliveira DA, Carvalho GM, Prado LB, Prado GF, Carvalho LB. Sleep-disordered breathing and orthodontic variables in children--pilot study. Int J Pediatr Otorhinolaryngol. 2014;78(11):1965-1969. doi: 10.1016/j.ijporl.2014.08.040. Epub 2014 Sep 6. PMID: 25242700.
- Centers for Disease Control and Prevention (CDC). National Center for Health Statistics (NCHS). Third National Health and Nutrition Examination Survey Data. Hyattsville, MD: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, July 1999, Available at [https://wwwn.cdc.gov/nchs/data/nhanes3/3a/VIFSE-acc.pdf].
- Grippaudo C, Paolantonio EG, Antonini G, Saulle R, La Torre G, Deli R. Association between oral habits, mouth breathing and malocclusion. Acta Otorhinolaryngol Ital. 2016;36(5):386-394. doi: 10.14639/0392-100X-770. PMID: 27958599; PMCID: PMC5225794.
- Souki BQ, Pimenta GB, Souki MQ, Franco LP, Becker HM, Pinto JA. Prevalence of malocclusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol. 2009;73(5):767-773. doi: 10.1016/j.ijporl.2009.02.006. Epub 2009 Mar 12. PMID: 19282036.
- Harari D, Redlich M, Miri S, Hamud T, Gross M. The effect of mouth breathing versus nasal breathing on dentofacial and craniofacial development in orthodontic patients. Laryngoscope. 2010;120(10):2089-2093.
- Pirilä-Parkkinen K, Pirttiniemi P, Nieminen P, Tolonen U, Pelttari U, Löppönen H. Dental arch morphology in children with sleep-disordered breathing, Eur J Orthod. 2009;31(2):160–167.
- Moorrees CF, Reed RB. Changes in dental arch dimensions expressed on the basis of tooth eruption as a measure of biologic age. J Dent Res. 1965;;44:129-141. doi: 10.1177/00220345650440010601. PMID: 14245926.
- Behrents RG, Shelgikar AV, Conley RS, et al. Obstructive sleep apnea and orthodontics: an american association of orthodontists white paper. Am J Orthod Dentofacial Orthop. 2019;156(1):13-28.e1.
- Incerti Parenti S, Fiordelli A, Bartolucci ML, Martina S, D'Antò V, Alessandri-Bonetti G. Diagnostic accuracy of screening questionnaires for obstructive sleep apnea in children: A systematic review and meta-analysis. Sleep Med Rev. 2021;57:101464.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted November 8, 2021
Submitted in final revised form April 13, 2022
Accepted for publication July 2, 2022
Address correspondence to: Kazuma Kitagaito, DMD, MSD, MSE 1959 NE Pacific St B-307, Seattle, WA 98195; Email: kazk@uw.edu