Letter 1, Issue 12.1
COMISA, Cardiometabolic Risk, and Other Critical Reasons for Considering Insomnia in Obstructive Sleep Apnea Treatment With Mandibular Advancement Devices
http://dx.doi.org/10.15331/jdsm.7378Miguel Meira e Cruz1, Fausto Pinto1, João Winck2
1Centro Cardiovascular da Universidade de Lisboa (CCUL@RISE), Faculdade de Medicina da Universidade de Lisboa, Lisboa, Portugal; 2 Faculdade de Medicina da Universidade do Porto, Porto, Portugal
Cardiometabolic (CM) diseases contribute, in a large proportion, to cardiovascular diseases, a leading cause of death worldwide.1 Accepting the critical role of sleep for cardiovascular (and related metabolic) health, the American Heart Association has recently updated the classic “Simple 7” to a contemporary form of the “Essential 8” supporting sleep duration as a mandatory aspect to be considered among other predictors of CM status.2 Insufficient sleep, sleep fragmentation, circadian misalignment, and chronodisruption are typical features presented by either patients with insomnia or those with sleep disordered breathing (SDB); the patients with SDB have more pronounced CM effects eventually related to nocturnal intermittent hypoxemic events because of the repetitive obstruction of the upper airway during sleep.3 All of these features are commonly associated with a short sleep duration. In addition, overweight/obesity, which is likely to occur in patients with obstructive sleep apnea (OSA), independently affects CM risk, sleep duration,4 and daytime functioning. An interaction among circadian timing system, insomnia, and OSA through CM dysfunction has also been suggested.5
Insomnia and OSA are indeed the most prevalent sleep disorders and the main reasons that patients present with sleep-related complaints. Interestingly, although OSA is usually identified as the primary sleep-related concern regarding CM risk, insomnia also is independently related to hypertension, diabetes, and other CM risk factors.6 Still, because these conditions are often concomitant, as in the case of comorbid insomnia and sleep apnea (COMISA), such interaction will further contribute to higher CM compromise7 and negatively influence other clinically relevant aspects of global health, such as circadian balance, higher brain functioning, vigilance, optimum performance during daytime hours, and psychosocial stress. For instance, patients with depression may present with higher risk for CM disturbances even with distinct phenotypic traits, leading some authors to propose a “cardiometabolic subtype of depression”.8 Following this concept, it is notable that some patients with COMISA experiencing high levels of psychosocial stress were found to benefit from cognitive behavioral strategies directed toward insomnia with effective results, not only for COMISA-related outcomes but also well-established CM risk factors.9 Also of great interest is our preliminary finding that patients with OSA who have sleep-onset insomnia as a common COMISA phenotype, respiratory status (assessed by the apnea-hypopnea index), insomnia (inferred by the polysomnography-based sleep latency ≥ 30 minutes), and autonomic balance as a surrogate of CM risk all showed marked improvements after treatment with a mandibular advancement device (MAD).9 However, insomnia may sometimes prove to be a significant challenge for patients with OSA, exhibited as difficulty with positive airway pressure, MAD, or compliance with conservative/ hygienic measures. The scope and relevance of those aspects concomitantly affect adults and a wide range of pediatric ages where COMISA is still prevalent and have a putative prognostic value for future CM risk.10 Though MAD therapy became critical in the modern practice of respiratory sleep medicine, an integrated approach for optimal management is often required. Specialists in the management of OSA should be aware of the risk factors, main clinical features, comorbid relationships, and general therapeutic strategies related to insomnia as the most frequent and often affecting OSA-comorbid sleep disorder. Yet, some constraints will be expected. For example, in some patients with low arousal threshold, insomnia may be exacerbated and thereby affect treatment success.11 Sex will eventually account for crucial clinical differences among symptoms and co-occurrences.12 However, insomnia with objective (but not subjective) short sleep duration (eg, <6 hours) was shown to increase the risk of hypertension.13 Given that major adverse cardiac events were observed to increase in older men with COMISA and in younger patients with obesity in controlled studies,14 age will likely play a role in the way insomnia interacts with OSA during a patient’s lifetime. These findings provide relevant implications, as follows: 1. Subjective measures of insomnia, valuable for other endeavors, may be less useful for identifying risk of CM morbidity and mortality warranting medical attention in patients presenting with sleep difficulties suggesting insomnia, and thus limit otherwise preventive actions. 2 Objective assessment of sleep duration by polysomnography is expensive and impractical. Therefore, other easy-to-use objective sleep tools such as wearable electronic records devices or sleep trackers may offer some benefit in this scope of practice, even though they should account for sex- and age-related specificities and clinical variability. 3 Effective treatment of patients with insomnia with short sleep duration relies on agents that are more likely to improve its pathophysiologic mechanisms, such as physiologic hyperarousal. For clinicians treating patients with OSA (particularly those using a MAD), and whenever insomnia is present (either from the sleep-onset, maintenance or sleep-offset type), taking into account clinical and polysomnographic phenotypes15 as well as environmental aspects and oriented behavioral strategies, together with adequate instrumental tools, should guide an efficient multicomponent treatment regimen with the goal to improve the general outcomes of this complex scenario.
In recent years, statements and guidelines from several dental sleep societies have been published regarding the practice of odontostomatology in the sleep medicine field, especially focusing on the management of MAD directed to patients with OSA. Therefore, recognizing the opportunity to magnify statements and recommendations on a particular topic and considering the great amount of evidence over the past few decades, particularly regarding the relationship between sleep disordered breathing, CM risk, and premature mortality, it seems acceptable to anticipate that the inclusion of insomnia will positively affect the standards of practice toward optimal and personalized care, favoring clinical, social, and financial outcomes. This also opens the door for additional research in this important field while positioning the dentist, together with other medical specialists, at the forefront of a gold standard primary care practice with the goal of better sleep.
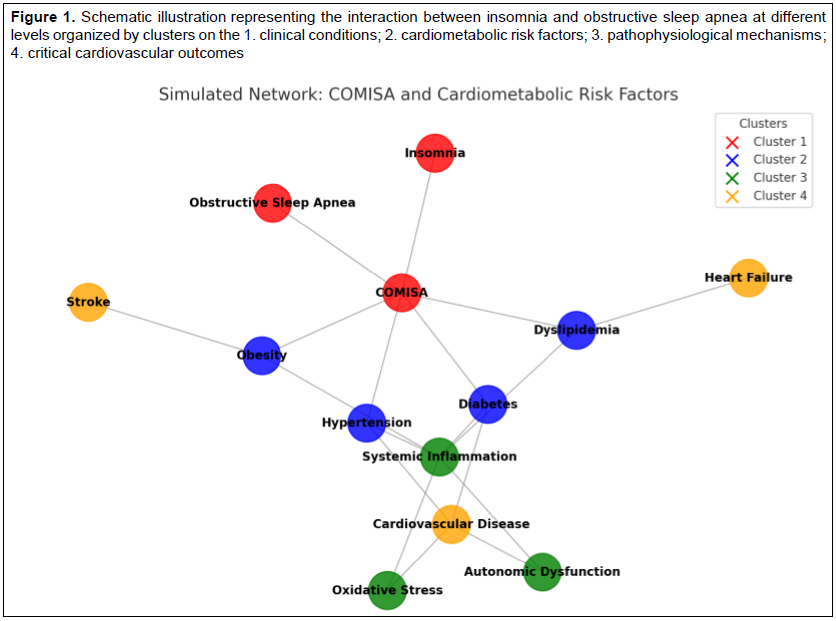
Figure 1Schematic illustration representing the interaction between insomnia and obstructive sleep apnea at different levels organized by clusters on the 1. clinical conditions; 2. cardiometabolic risk factors; 3. pathophysiological mechanisms; 4. critical cardiovascular outcomes |
{kind=link}
CITATION
Meira e Cruz M, Pinto F, Winck J. COMISA, cardiometabolic risk, and other critical reasons for considering insomnia in obstructive sleep apnea treatment with mandibular advancement devices. J Dent Sleep Med. 2025;12(1).REFERENCES
- Tsao CW, Aday AW, Almarzooq ZI, et al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2023 Update: A Report From the American Heart Association. Circulation. 2024;147(8):e93–e621. https://doi.org/10.1161/CIR.0000000000001123
- Makarem, N., Castro-Diehl, C., St-Onge, MP, et al. Redefining cardiovascular health to include sleep: Prospective associations with cardiovascular disease in the MESA Sleep Study. J Am Heart Assoc. 2022;11(21):e025252. https://doi.org/10.1161/JAHA.122.025252
- André S, Andreozzi F, Van Overstraeten C, et al. Cardiometabolic comorbidities in obstructive sleep apnea patients are related to disease severity, nocturnal hypoxemia, and decreased sleep quality. Respir Res. 2020;21(1):35. doi: 10.1186/s12931-020-1284-7. PMID: 31996224; PMCID: PMC6990595.
- Amiri S. Body mass index and sleep disturbances: A systematic review and meta-analysis. Postep Psychiatr Neurol. 2023;32(2):96-109. doi: 10.5114/ppn.2023.129067. Epub 2023 Jun 28. PMID: 37497197; PMCID: PMC10367528.
- Meira E Cruz M, Gozal, D. Sleepiness and cardiometabolic impact of short sleep duration and OSA: What about the clock? Chest. 2019;156(6), 1273–1274. https://doi.org/10.1016/j.chest.2019.07.029
- Nobre B, Rocha I, Morin CM, Cruz MME. Insomnia and circadian misalignment: an underexplored interaction towards cardiometabolic risk. Sleep Sci. 2021;14(1):55-63. doi: 10.5935/1984-0063.20200025. PMID: 34104338; PMCID: PMC8157774.
- Meira E Cruz M, Salles C, Gozal, D. A reappraisal on the associations between sleep-disordered breathing, insomnia, and cardiometabolic risk. Am J Respir Crit Care Med. 2021;203(12): 1583–1584. https://doi.org/10.1164/rccm.202102-0337LE
- Geraets AF, Schram J, Jansen MT, et al. The cardiometabolic depression subtype and its association with clinical characteristics: The Maastricht Study. J Affect Dis.2022;313:110-117. https://doi.org/10.1016/j.jad.2022.06.045
- Meira e Cruz M, Brito, R, Rocha I, et al. Clinically guided digital cognitive behavioural therapy for insomnia (CBTi) in patients with COMISA: A case-control pilot study with focus on mental health and cardiometabolic risk factors. Sleep Med. 2024;115(1):S165. https://doi.org/10.1016/j.sleep.2023.11.472.
- Meira E Cruz M. Comorbid insomnia and sleep apnea: COMISA. Dent Clin North Am. 2024;68(3):455–466. https://doi.org/10.1016/j.cden.2024.03.002
- Antonaglia C, Vidoni G, Contardo L, et al. Low arousal threshold estimation predicts failure of mandibular advancement devices in obstructive sleep apnea syndrome. Diagnostics (Basel, Switzerland), 2022;12(10):2548. https://doi.org/10.3390/diagnostics12102548
- Mysliwiec V, Pruiksma KE, Matsangas P, et al; STRONG STAR Consortium. Sex differences in US military personnel with insomnia, obstructive sleep apnea, or comorbid insomnia and obstructive sleep apnea. J Clin Sleep Med. 2024;20(1):17–30. https://doi.org/10.5664/jcsm.10774
- Dai Y, Chen B, Chen L, et al. Insomnia with objective, but not subjective, short sleep duration is associated with increased risk of incident hypertension: the Sleep Heart Health Study. J Clin Sleep Med. 2023;19(8):1421-1428. doi: 10.5664/jcsm.10570. PMID: 37078185; PMCID: PMC10394371.
- Fang F, Sun Z, Gao Y, et al. Effects of combined morbid insomnia and sleep apnea on long-term cardiovascular risk and all-cause mortality in elderly patients: A prospective cohort study. BMC Geriatr. 2024;24(1):622. https://doi.org/10.1186/s12877-024-05147-2
- Manetta IP, Duarte BB, Nucci LB, Enes CC. Relationship between OSA pathophysiological phenotypes and treatment response to mandibular advancement devices: a pilot study. J Clin Sleep Med. 2024;20(8):1321–1330.
SUBMISSION AND CORRESPONDENCE INFORMATION
Submitted for publication August 23, 2024Accepted for publication September 2, 2024
Address correspondence to: Dr. Miguel Meira e Cruz; Email: mcruz@medicina.ulisboa.pt