Case Report, Issue 7.3
Patient With Severe Obstructive Sleep Apnea Treated With the Orthoapnea Mandibular Advancement Device: A Case Report
http://dx.doi.org/10.15331/jdsm.7132
Pedro Mayoral DDS MSc PhD1, Manuel O Lagravère DDS MSc PhD2, Manuel Miguez DDS MSc PhD3
1Catholic University of Murcia UCAM, Director Master Program Dental Sleep Medicine, Madrid, Spain; 2University of Alberta, Faculty of Medicine and Dentistry, School of Dentistry, Alberta Canada; 3Catholic University of Murcia UCAM, Dental Sleep Medicine Program, Madrid, Spain
ABSTRACT
The objective of this case report is to show success of mandibular advancement device (MAD) in an adult patient with OSA. Sleep disturbances affect > 50% of individuals 65 years or older. OSA is one of these. This case was conducted with a male patient who was 65 years old and had severe apnea (AHI 45.5). After six weeks of using MAD, AHI was reduced to 4.3. MAD improved and controlled OSA which reflected to a better quality of life of the patient.
Keywords:
Mandibular Advancement Device, Cone-Beam Computed Tomography, Obstructive Sleep Apnea
Citation:
Mayoral P, Lagravère MO, Miguez M. Patient with severe obstructive sleep apnea treated with the orthoapnea mandibular advancement device: A case report. J Dent Sleep Med. 2020;7(3)
INTRODUCTION
Sleep complaints are common in the elderly, with reports indicating that individuals aged 65 years or older have sleep disturbances that affect more than 50% of them.1 Obstructive sleep apnea (OSA) is one of the most common sleep disturbances and a serious public health problem in which complete or partial obstruction of the upper airway during sleep results in sleep fragmentation and oxygen desaturation.2 The nocturnal hypoxemia and sleep fragmentation can cause excessive daytime sleepiness, poor concentration, and hypertension.2
Mandibular advancement devices (MAD) are an effective treatment for OSA.3 These appliances increase the width of the airway and reduce its collapsibility by keeping the mandible in a protruded position during sleep. The American Academy of Sleep Medicine (AASM) recommends the use of oral appliances in patients with snoring, mild to moderate OSA, or severe OSA who are intolerant of continuous positive airway pressure (CPAP) therapy or prefer alternate therapy.4
The design features of the MAD have a major influence on patient tolerance, compliance, and success rate.5 The key features are the extension, retention, and material of the upper and lower splints, the coupling mechanism that keeps the mandible forward while sleeping, and the mechanism to titrate or advance the mandible even more when necessary.5
There are numerous differences in the design of commercially available MADs. Certain appliances have coupling mechanisms that allow the mouth to open while sleeping, bringing the mandible backward and losing part of the advancement and therefore the efficacy.6-8 Finally, there are appliances that increase the vertical dimension by excessively reducing the range of mandibular advancement.9 The main causes for discontinuation of MAD therapy are reportedly that the appliance is ‘‘bothersome to use’’, and has ‘‘little or no effect’’ in preventing sleep apnea, which is largely caused by a design problem or selection of the wrong type of appliance.10
The MAD Orthoapnea (Ortoplus, Málaga, Spain) is a two-piece, custom-made, adjustable device that allows good occlusal contact while the patient is in the rest position. It also permits lateral and vertical jaw movement during sleep, and controlled regulation of the mandibular advancement reducing apnea-hypopnea index (AHI) and controlling the signs and symptoms of OSA.6
REPORT OF CASE
A male patient 65 years old, with severe apnea (AHI 45.5) presented to the clinic in March 2016. He reported loud snoring, three to four awakenings during the night, nocturnal polyuria two to three times per night, frequent morning headaches, and excessive daytime sleepiness that affected his daily, professional and social life. Polysomnography showed mild desaturation (5% SaO2<90%, 81 lowest SaO2). History indicated that the patient does not tolerate treatment with CPAP. CPAP was recommended by a sleep physician and initiated in December 2015, but after 3 months the patient refused to continue because of intolerance related to the excessive air pressure (16 cm/H20) and problems with the mask.
An alternative treatment was planned, which consisted of the use of a MAD. The patient was examined by the dentist to determine the suitability for a MAD, and then proper medical and dental histories were taken, and consent forms were signed. The patient provided full orthodontic records, and upper and lower polyvinyl siloxane impressions, intraoral/extraoral photographs (Figure 1), and cone beam computed tomography images were obtained (Figure 2) (Carestream CS 9300 Select, Rochester, NY exposition 80Kv 4mA 8,01s, dose 448mGy cm2, size 18µmx18µmx18µm, image 10cmx10cmx10cm). We used a convention workflow and George gauge (Great Lakes Orthodontics, New York, New York, USA) to obtain a polyvinyl siloxane bite registration. Each physical impression was poured and articulated with the bite. We then examined the bite to ensure there was a sufficient vertical gap (> 3 mm) to enable manufacture of the MAD Orthoapnea. The amount of mandibular advancement initially was 67% (8 mm) 4 and the amount of bite opening was 5 mm between the upper and lower incisor tip. These amounts are the standard protocol used with these appliances. In our patient, it was necessary to provide progressive mandibular advancement up to 9 mm until improvement or resolution of symptoms (titration process), leading to a significant reduction or disappearance of subjective and objective symptoms of OSAS such as witnessed apneas, snoring, and excessive daytime sleepiness, and an improved AHI. Titration with this appliance was easy to do and was controlled by the doctor and patient.
Figure 1Intraoral photographs. A, Right, frontal, and left views without the MAD device. B, Right, frontal, and left views with the MAD Orthoapnea device. C, Right and frontal views showing maximum opening allowed with the MAD in place. |
{kind=link}
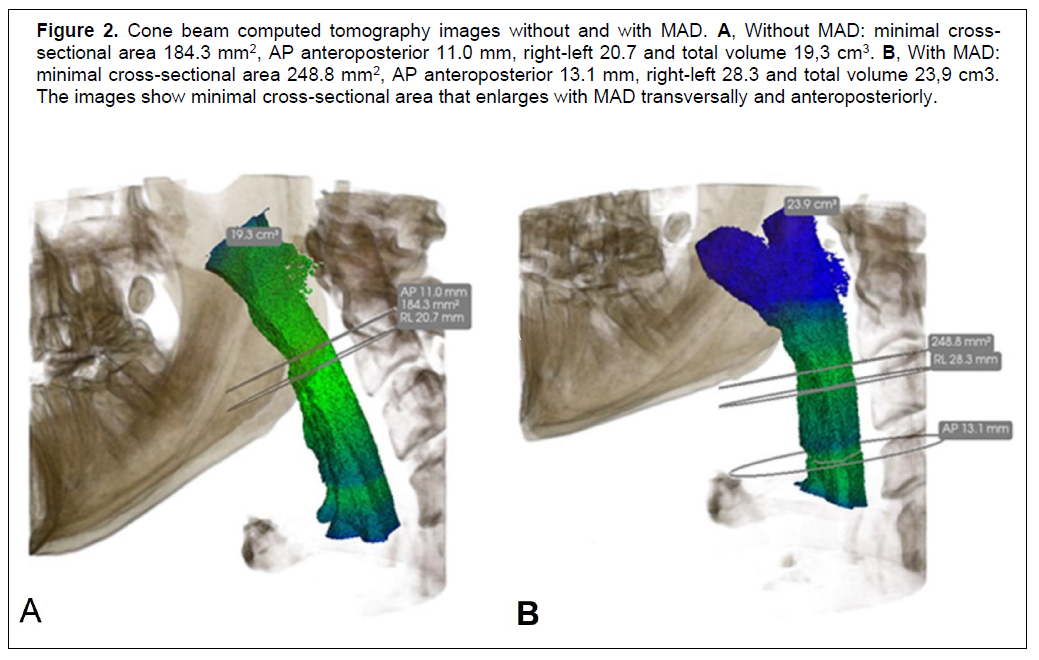
Figure 2Cone beam computed tomography images without and with MAD. A, Without MAD: minimal cross-sectional area 184.3 mm2, AP anteroposterior 11.0 mm, right-left 20.7 and total volume 19,3 cm3. B, With MAD: minimal cross-sectional area 248.8 mm2, AP anteroposterior 13.1 mm, right-left 28.3 and total volume 23,9 cm3. The images show minimal cross-sectional area that enlarges with MAD transversally and anteroposteriorly. |
{kind=link}
The patient received the appliance and was instructed in its use. The dentist made the adjustment needed: the inside surface was adjusted to fit the teeth as well as the occlusal surfaces to achieve properly balanced occlusion. Follow-up controls were made at 1, 3, and 6 weeks afterward. Intraoral and extraoral photographs were taken with the MAD (Figure 1), as well as cone beam computed tomography (Carestream CS 9300 Select) after 6 weeks with the patient using the MAD to measure airway area and volume (Figure 2).
The success of the appliance is explained by the possibility to adjust the protrusion and limit and control the opening of the mandible during sleep. The good adaptation and tolerance to it is because of the occlusal stability and the possibility of presenting physiological movements at opening and lateral movements.
After 6 weeks of using the device, the patient showed significant improvement, with AHI reduced to a normal value of 4.3 events/h with no snoring, no waking up during the night, no nocturnal polyuria, reduction of the morning headaches, and improved concentration. This patient is still using the appliance 12 months later.
DISCUSSION
This case demonstrates that the MAD is an effective treatment alternative for patients with OSA as proposed by the Clinical Practice Guidelines of the AASM.4 The result in this case is similar to the study of Romero6 and confirms the efficacy and good tolerance of the Orthopnea MAD.
The design of this appliance has several advantages compared to other devices. The MAD used is made of two mouthpieces that cover all the teeth with a soft inner material that provides good retention and comfort; the outer part is hard and provides strength and good occlusal stability. The coupling mechanism is an inverted rod screw that permits a controlled regulation of the mandibular advancement, allows lateral and vertical jaw movement during sleep, and limits opening to 10 mm without retrusion of the mandible (Figure 1). Milano et al7 and Norrhem et al8 mention that control of the opening significantly increases the success of the MAD.
The effects of treatment on health outcomes have been demonstrated with the use of MAD Orthoapnea in this patient. Subjective daytime sleepiness, assessed by the Epworth Sleepiness Scale, improves with the MAD as seen in our patient. The patient presented with severe somnolence during the day and reported that it affected his professional activity and daily normal life. After 6 weeks of appliance usage, the problems were eliminated. Other frequent symptoms of OSA seen in this patient were nocturnal polyuria, night awakening, and morning headaches. The MAD treatment showed significant improvement and control of these symptoms and this translates to a better quality of life for patients.3
REFERENCES
- Neikrug AB, Ancoli-Israel S. Sleep disorders in the older adult - a mini-review. Gerontology. 2010;56(2):181–189.
- Telakivi T, Kajaste S, Partinen M, Koskenvuo M, Salmi T, Kaprio J. Cognitive function in middle-aged snorers and controls: Role of excessive daytime somnolence and sleep-related hypoxic events. Sleep. 1988;11(5):454-462.
- SerraTorres S, BellotArcís C, MontielCompany JM, MarcoAlgarra J, AlmerichSilla JM. Effectiveness of mandibular advancement appliances in treating obstructive sleep apnea syndrome: a systematic review. Laryngoscope. 2016;126(2):507-514.
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773-827.
- Sutherland K, Vanderveken OM, Tsuda H, et al. Oral appliance treatment for obstructive sleep apnea: an update. J Clin Sleep Med. 2014;10(2):215-227.
- Romero, MM, Samalea PV, César EC, Marfil NR, Sánchez MCV. Efficacy of Orthoapnea Mandibular Advance Device in Patients with Mild and Moderate Obstructive Sleep Apnea Syndrome. J Sleep Med Disord. 2016;3(6):1065.
- Milano F, Mutinelli S, Sutherland K, et al. Influence of vertical mouth opening on oral appliance treatment outcome in positional obstructive sleep apnea. J Dental Sleep Med. 2018;5(1):17–23.
- Norrhem N, Nemeczek H, Marklund M. Changes in lower incisor irregularity during treatment with oral sleep apnea appliances. Sleep Breath. 2017;21(3):607-613.
- Mayoral P, Lagravere MO, Miguez-Contreras M, Garcia M. Antero-posterior mandibular position at different vertical levels for mandibular advancing device design. BMC Oral Health. 2019;19(1):85
- Nishigawa K, Hayama R, Matsuka Y. Complications causing patients to discontinue using oral appliances for treatment of obstructive sleep apnea. J Prosthodont Res. 2017;61(2):133-138
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication June 3, 2019
Submitted in final revised form February 24, 2020
Accepted for publication April 6, 2020
Address correspondence to: Manuel Lagravère, DDS MSc PhD, University of Alberta, Faculty of Medicine and Dentistry, School of Dentistry, ECHA 5-524, 11405-87 Avenue, Edmonton, Alberta T6G 1C9, Canada; email: mlagravere@ualberta.ca