Case Report, Issue 2.4
Severe Obstructive Sleep Apnea Treated with Combination Hypoglossal Nerve Stimulation and Oral Appliance Therapy
http://dx.doi.org/10.15331/jdsm.5124
Jake J. Lee, BS1 ; Nivedita Sahu, MD2 ; Robert Rogers, DMD, DABDSM3 ; Ryan J. Soose, MD2
1University of Pittsburgh School of Medicine, Pittsburgh, PA; 2UPMC Department of Otolaryngology, Pittsburgh, PA; 3Pittsburgh Dental Sleep Medicine, Wexford, PA
Abstract
Hypoglossal cranial nerve stimulation therapy via an implantable neurostimulation system is a promising new therapy for moderateto-severe obstructive sleep apnea patients who are unable to adhere to positive pressure therapy and who meet certain anatomical and clinical characteristics. Treatment for non-responders or incomplete responders to this novel therapy has not been studied. Particularly for patients who fail positive pressure therapy, a management plan combining multiple treatment modalities is increasingly common. This case report highlights a participant from the multicenter Inspire STAR trial who previously failed to achieve benefit with oral appliance monotherapy but then subsequently reintroduced oral appliance therapy successfully in an adjunctive role to augment the effectiveness of hypoglossal nerve stimulation therapy. Discussion will focus on the factors associated with design and selection of the oral appliance as well as the electrical parameters and titration of the neurostimulation in this unique clinical situation.Keywords:
sleep apnea, oral appliance, hypoglossal nerve stimulation, combination therapy, inspire therapyCitation:
Lee JJ, Sahu N, Rogers R, Soose RJ. Severe obstructive sleep apnea treated with combination hypoglossal nerve stimulation and oral appliance therapy. Journal of Dental Sleep Medicine 2015;2(4):185–186.Hypoglossal nerve stimulation (HNS) using the Inspire neurostimulation system (Inspire Medical Systems, Minneapolis, MN) is an emerging treatment modality for obstructive sleep apnea (OSA), involving synchronization of tongue protrusor stimulation and ventilatory effort during sleep. In a prospective multicenter trial, participants who met specific clinical and anatomical inclusion criteria had significant improvements in subjective and objective OSA outcome measures, and the treatment effect was maintained at long-term follow-up.1,2 There is no literature, however, on management of partial responders. This case report details the combination of HNS and oral appliance therapy (OAT) to successfully treat severe OSA after incomplete response with either treatment in isolation.
REPORT OF CASE
A 75-year-old male presented with a 12-year history of severe OSA. Sleep-related symptoms included loud disruptive snoring, witnessed apnea, nocturnal awakenings, and unrefreshing sleep. Although CPAP therapy provided years of subjective and objective improvement, he sought alternative treatment options due to multiple mask- and pressure-related side effects, persistent equipment-related nocturnal awakenings, and cumbersomeness with travel and camping. Oral appliance monotherapy with a custom mandibular repositioning device (TAP, Airway Labs, Carrollton, TX) was initiated two years prior to presentation, but inadequate symptom improvement and discomfort resulted in discontinuation (prior to repeat sleep testing). He later enrolled in the Inspire STAR Trial and underwent implantation of the HNS system after meeting the study inclusion criteria.1
Baseline STAR Trial diagnostic polysomnography (PSG) showed an AHI of 43.7, lowest arterial oxygen saturation (LSAT) of 75%, and arterial oxygen saturations below 90% (T90) for 33.8% of total sleep time. Six months after implantation, PSG with HNS therapy showed significant reduction in sleep apnea severity with an AHI of 11.6, LSAT 82%, and T90 of 10.2%. Patient-reported measures of daytime sleepiness and sleep-related quality of life were in the normal range at baseline and remained unchanged with HNS therapy. Per self-report and bedpartner report, snoring was significantly reduced with treatment from “loud/bedpartner leaves room” to “soft” on a visual analog scale but was not completely eliminated.
Over the subsequent year, attempts to further augment the effectiveness of HNS were made by the sleep physician/surgeon with positional therapy, topical nasal therapy, and adjustment of the electrical stimulation parameters. Although clinical, PSG, and satisfaction outcome measures remained significantly improved with nightly HNS use, mild OSA and bothersome snoring persisted.
The patient was then refitted with a new mandibular repositioning device to augment the HNS therapy. The Medley Gold (see Figure 1; TMD Technologies, Lilburn, GA) appliance was selected to allow increased anterior space for tongue protrusion that occurs with HNS therapy. Accommodation to the new appliance was successful with good subjective adherence; however, he developed intraoral discomfort, reporting that the stimulation now was too strong with combination therapy. OAT alone (HNS turned off) was tried for several weeks but again sleep-related symptoms, including loud snoring, recurred. The patient then underwent HNS reprogramming with the oral appliance in place to reduce stimulation amplitude (1.3V to 0.8V) and improve comfort.
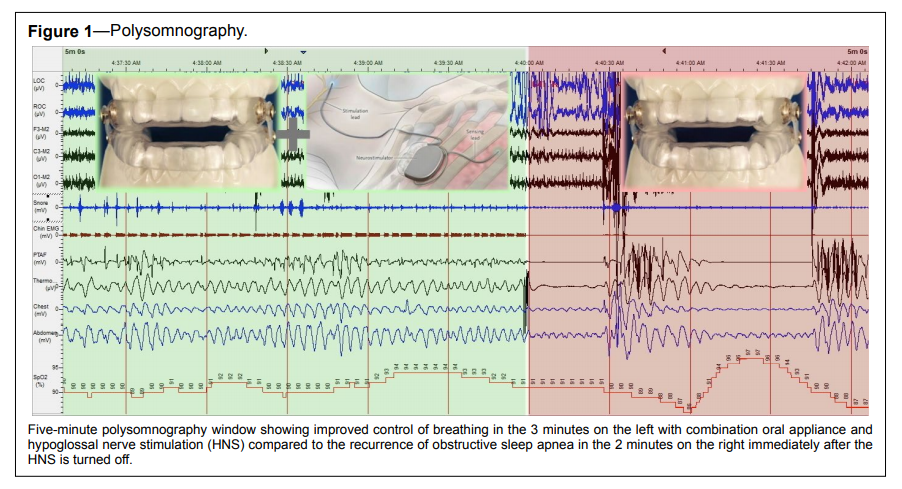
Figure 1Polysomnography. |
{kind=link}
Combination therapy with the new Medley Gold appliance and reduced HNS settings resulted in excellent subjective adherence and clinical improvement including resolution of snoring. A new PSG was completed with combination therapy. Early in the study, HNS was wirelessly turned off to assess the effect of OAT alone (18.6 min) with clear return of sleep-disordered breathing and an AHI of 29.2 during this time. HNS therapy was then re-activated for the remainder of the night (286.9 min) during which combination therapy resulted in an AHI of 2.1 (Figure 1). The final PSG report for the entire night (305.5 min) confirmed complete objective control, with an overall AHI of 3.5, LSAT 86%, and T90 of 0.8%.
DISCUSSION
Interdisciplinary collaboration with multimodality treatment is an increasingly common approach particularly for severe OSA, although guidelines on patient phenotyping, sequencing of treatment, and specific algorithms are still lacking in the literature.3–5 In this first reported case of combination OAT and HNS therapy, symptoms and objective control of breathing were normalized as compared to partial OSA improvement with each in isolation. Furthermore, both the HNS stimulation amplitude and the degree of mandibular advancement could be reduced compared to when each was used as monotherapy. Two key learning points may be noted in this case: (1) Stimulation parameters may be reduced on the HNS system with introduction of OAT, perhaps analogous to prior reports of reduced CPAP requirements with combination CPAP and OAT.4,5 (2) An oral appliance design with sufficient anterior room to accommodate tongue protrusion during active stimulation should be considered in HNS patients.
REFERENCES
2. Strollo PJ, Gillespie MB, Soose RJ, et al. Upper airway stimulation for obstructive sleep apnea: durability of the treatment effect at 18 months. Sleep 2015 Jun 22. [Epub ahead of print].
3. Vanderveken OM. Combination therapy for obstructive sleep apnea in order to achieve complete disease alleviation: from taboo to new standard of care. J Dent Sleep Med 2015;2:7–8.
4. El-Solh AA, Moitheennazima B, Akinnusi ME, Churder PM, Lafornara AM. Combined oral appliance and positive airway pressure therapy for obstructive sleep apnea: a pilot study. Sleep Breath 2011;15:203–8.
5. Eaton MJ, Tucker JH. Combination therapy of oral appliance and autotitrating CPAP of patient with edentulous maxillary arch. J Dent Sleep Med 2015;2:127–8.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication August, 2015Accepted for publication August, 2015
Address correspondence to: Ryan J. Soose, MD, Director, UPMC Division of Sleep Surgery, Department of Otolaryngology, UPMC Mercy Building B, Suite 11500; 1400 Locust Street, Pittsburgh, PA 15219; Tel: (412) 232-8989; Fax: (412) 232-8525; Email: sooserj@upmc.edu
DISCLOSURE STATEMENT
Funding for the STAR Trial provided by Inspire Medical Systems. Robert Rogers is the inventor of the Medley Gold oral appliance. Dr. Soose is a STAR Trial investigator and has consulted for Inspire Medical Systems and Philips-Respironics. The other authors have indicated no financial conflicts of interest. There was no off-label or investigational use.
PDF