Case Report 3, Issue 7.3
The Use of a Passive Tongue Restraint Device With Moisture Bubble to Treat Obstructive Sleep Apnea in a Case Contraindicated for Mandibular Advancement Splint Therapy
http://dx.doi.org/10.15331/jdsm.7136
Gregory Turek, BDS (Syd)
Somcentre Dental Sleep Medicine Clinic, Sydney, NSW, Australia
ABSTRACT
This report describes the use of a Tongue Tamer (TT) device for passive tongue restraint in an 85-year-old woman with moderately severe obstructive sleep apnea. Device treatment options were limited; continuous positive airway pressure therapy had failed and mandibular advancement splint (MAS) therapy was contraindicated in this patient. Previous use of the TT in patients with incomplete response to MAS therapy showed further reduction of the apnea-hypopnea index. However, use of the TT has not been assessed without mandibular advancement. A lower occlusal splint was made with TT frames added, and a "moisture bubble" for the tongue to sit in also was provided. The patient tolerated the TT well and reported her tongue was in the retaining device upon waking in the morning. The apnea-hypopnea index reduced from 27.5 to 17.5 events/h on a follow-up sleep study with the TT. This novel method of passive restraint of the tongue may provide some benefit when MAS therapy is not possible.
Keywords:
Obstructive sleep apnea; Oral appliance; tongue; alternative therapy
Citation:
Turek G. The use of a passive tongue restraint device with moisture bubble to treat obstructive sleep apnea in a case contraindicated for mandibular advancement splint therapy. J Dent Sleep Med. 2020;7(3)
INTRODUCTION
Stabilization of the tongue is a therapeutic target for obstructive sleep apnea (OSA). Tongue retaining devices, which hold the tongue anteriorly using suction forces, have a demonstrated effect as a type of therapy for OSA, reducing apnea-hypopnea index (AHI) by approximately 50%.1 This is similar to the average AHI reduction following mandibular advancement splint (MAS) therapy.2 However, active tongue restraint using a suction bulb is associated with significant discomfort and hence poor usage.3
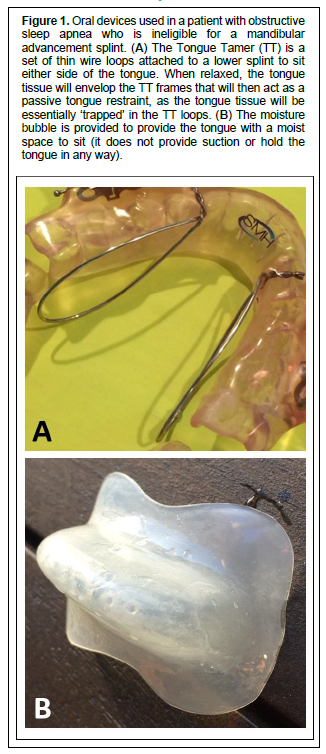
An alternative approach to tongue restraint is through ‘passive’ means using a device called the Tongue Tamer (TT).4 The TT is a uniquely shaped set of thin wire frames that attach to a lower dental splint, sitting on either side of the tongue (Figure 1A). The concept is that a relaxed tongue with minimal muscle tone would envelop the loops created by the TT frames. The tongue tissue within the TT loops would act to restrain the tongue and prevent posterior movement of the tongue into the airway. The TT has previously been assessed as an adjunct to the MAS in a case series of 17 patients with OSA with an incomplete response to MAS therapy.4 A repeat sleep study with the TT added to the lower plate of the MAS showed on average an additional 40% reduction in AHI compared to MAS therapy alone.4 This report describes the use of the TT as a tongue restraining device only (without mandibular advancement) in an individual with temporomandibular joint (TMJ) contraindications for MAS therapy.
Figure 1Oral devices used in a patient with obstructive sleep apnea who is ineligible for a mandibular advancement splint. (A) The Tongue Tamer (TT) is a set of thin wire loops attached to a lower splint to sit either side of the tongue. When relaxed, the tongue tissue will envelop the TT frames that will then act as a passive tongue restraint, as the tongue tissue will be essentially ‘trapped’ in the TT loops. (B) The moisture bubble is provided to provide the tongue with a moist space to sit (it does not provide suction or hold the tongue in any way). |
{kind=link}
REPORT OF CASE
This case study is of an 85-year-old woman with moderately severe OSA (AHI = 27.5/h, in-laboratory polysomnography) and obesity (body mass index 34.2 kg/m2). She was intolerant of continuous positive airway pressure and was referred by her sleep physician to a dentist for an adjustable MAS. She attended the Somcentre Dental Sleep Medicine clinic (Sydney, Australia). Dental examination revealed TMJ issues and the patient was concerned about her “jaw pain issues” in relation to MAS therapy, as well as risk to existing dental work. Because of these issues, the patient was not receptive to using a MAS and therefore it was not an option. Hence, tongue restraint was performed and a TT device implemented. A Som Brux lower occlusal splint was made, to which the TT frames were added. The TT frames were made from 0.8-mm-diameter round orthodontic wire in an elongated loop shape and added to the splint (Figure 1A). In addition, the patient was provided with a moisture bubble to wear simultaneously (Figure 1B). The moisture bubble was provided to keep the tongue tip moist for comfort, by providing a pseudo lip seal. The moisture bubble was formed from soft, thin bleaching tray material and a vacuum formed over an appropriately sized tongue tip-shaped plaster cast. This bubble does not hold the tongue (it is not a suction bulb) and provides no mechanism by which the tongue could be ‘captured’ in a forward position, but provides a moist space for the tongue tip. The vertical opening provided by the TT device and moisture bubble is relatively minimal (1.5-mm splint thickness + 3 to 6 mm for tongue tip). At follow-up, the patient reported that the device was easy to wear, and was able to wear it all night. She reported that her tongue was still within the frames of the TT retaining device upon waking in the morning, suggesting that the tongue tissue had enveloped the TT loops, creating a passive tongue restraint. The sleep physician referred her for a follow-up sleep study wearing the TT device, 7 months later. The sleep study results are shown in Table 1.
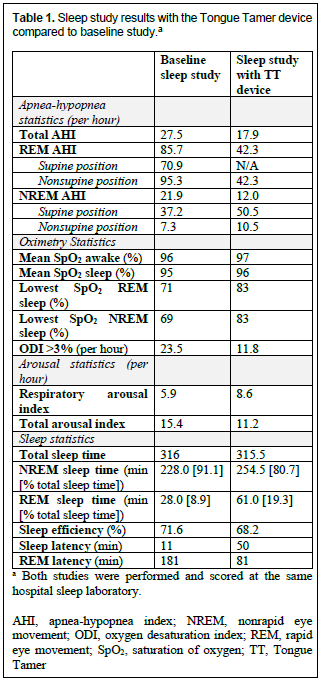
The TT study shows an improvement in AHI of approximately 10 events/h, bringing the patient closer toward mild OSA (AHI < 15 events/h). There was a corresponding improvement in oxygen desaturation index and lowest oxygen saturation rising from 69% in nonrapid eye movement and 71% in rapid eye movement (REM) sleep to 83%. There was also an improvement in REM sleep time and REM sleep latency.
Table 1Sleep study results with the Tongue Tamer device compared to baseline study.a |
{kind=link}
DISCUSSION
Most tongue restraint methods rely on active forces such as gripping, pressing, electrical stimulation, or suction.3 The TT is a different method of tongue restraint, using the natural passive ‘flow’ of the tongue to fill any surface or shape in low muscle tone conditions (sleep) to allow it to be passively restrained. The idea is that this type of tongue restraint would be more comfortable than the aforementioned active restraint methods, although no comparative studies exist at this stage. Results from an investigation of a series of 17 patients with an incomplete response to the MAS and failure of continuous positive airway pressure indicated a benefit of the TT over MAS therapy alone.4 In this case, the woman was ineligible for MAS therapy because of TMJ issues, so the TT was trialed as a single OSA therapy. The patient reported finding the device easy to wear. Although residual OSA was still evident on the follow-up sleep study, there was evidence of benefit and in a case with no other treatment options, a positive outcome can be seen. This is a single case of tongue restraint with TT without mandibular advancement. Further evidence is needed but this method could prove to be a useful addition to the treatment armamentarium of the dental sleep medicine clinician.
REFERENCES
- Chang ET, Fernandez-Salvador C, Giambo J, et al. Tongue retaining devices for obstructive sleep apnea: A systematic review and metaanalysis. Am J Otolaryngol. 2017;38(3):272-278.
- Sutherland K, Takaya H, Qian J, Petocz P, Ng AT, Cistulli PA. Oral appliance treatment response and polysomnographic phenotypes of obstructive sleep apnea. J Clin Sleep Med. 2015;11 (8):861-868.
- Deane SA, Cistulli PA, Ng AT, Zeng B, Petocz P, Darendeliler MA. Comparison of mandibular advancement splint and tongue stabilizing device in obstructive sleep apnea: a randomized controlled trial. Sleep. 2009;32(5):648-653.
- Turek G. A novel device for passive restraint of the tongue as an adjunct to mandibular advancement therapy in incomplete responders. J Dent Sleep Med. 2019;6(2).
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication July 16, 2019
Submitted in final revised form January 14, 2020
Accepted for publication February 3, 2020
Address correspondence to: Gregory Turek, BDS (Syd), Somcentre Dental Sleep Medicine Clinic, Level 3, 20 Clarke St Crows Nest NSW 2065, Australia; Tel: +61 2 9467 0400; Fax: +61 2 9467 0467; E-mail: gregoryturek@optusnet.com.au