Case Report 3, Issue 3.2
A Pitfall of an Orthodontic Approach to Pubescent Obstructive Sleep Apnea: A Case Report
http://dx.doi.org/10.15331/jdsm.5726
Keiko Maeda, PhD1,2,3,4; Eiki Itoh, PhD1,2,3,4; Yoko Okawara, DDS1 ; Yoichiro Takei, RPSGT2 ; Mina Kobayashi, PhD1,2,4; Yuichi Inoue, PhD1,2,3,4; Satoru Tsuiki, PhD1,2,3,4
1 Japan Somnology Center, Institute of Neuropsychiatry, Tokyo, Japan; 2 Yoyogi Center for Sleep Disorders, Tokyo, Japan; 3Department of Somnology, Tokyo Medical University, Tokyo, Japan; 4Foundation of Sleep and Health Sciences, Tokyo, Japan
ABSTRACT
Orthodontic treatment has potential as a fundamental approach in pubescent obstructive sleep apnea (OSA) patients with a small mandible. However, pitfalls of such treatment have not been documented. We report the case of a 15-year-old OSA patient (apnea hypopnea index [AHI] = 7.6 events/h) with a small mandible in whom we attempted to improve OSA by promoting the growth of the mandible with a mandibular advancement device. The AHI was reduced to 0.8 events/h with the device in place. However, neither notable growth of the mandible nor improvement of OSA without the device in place was observed after a 5-year follow-up (AHI = 7.8 events/h). It was retrospectively concluded that the optimal timing as an orthodontic treatment had already passed when the patient was introduced to our clinic. Hence, an orthodontic approach should be considered as soon as we encounter pubescent OSA so as not to lose an available window for definitive treatment.
Keywords:
obstructive sleep apnea, pubescent OSA, orthodontic treatment
Citation:
Maeda K, Itoh E, Okawara Y, Takei Y, Kobayashi M, Inoue Y, Tsuiki S. A pitfall of an orthodontic approach to pubescent obstructive sleep apnea: a case report. Journal of Dental Sleep Medicine 2016;3(2):73–74.
INTRODUCTION
If the patient’s predisposing factor for obstructive sleep apnea (OSA) is associated with a small mandible, the use of a mandibular advancement device (MAD) as an orthodontic approach is reasonable because nightly use of this device efficiently facilitates the growth of the mandible as long as patients are in the pubescent period, when mandibular growth can be expected in parallel with somatic growth.1–3 Conversely, we recently experienced a case who was treated by an MAD but did not show either a fundamental improvement of OSA or growth of the mandible. This case highlights a potential pitfall of an orthodontic approach to pubescent OSA unless it is provided at a particular timing.
REPORT OF CASE
A 15-year-old boy was diagnosed with mild OSA (apneahypopnea index [AHI] = 7.6 events/h), and was referred for oral appliance therapy using an MAD in our Sleep Apnea Dental Clinic. The patient had complained of frequent dozing off during school classes, chronic fatigue, and difficulty in waking up in the morning. His family reported loud snoring with episodes of apneas. His father was an untreated snorer who had experienced witnessed apneas. The score on the Japanese version of the Epworth Sleepiness Scale (JESS) at the patient’s first visit was 13.4 He had a thin physique with a BMI of 17.4 kg/m2 . There was no hypertrophy of the tonsil or adenoidal tissue, and no chronic nasal obstruction.
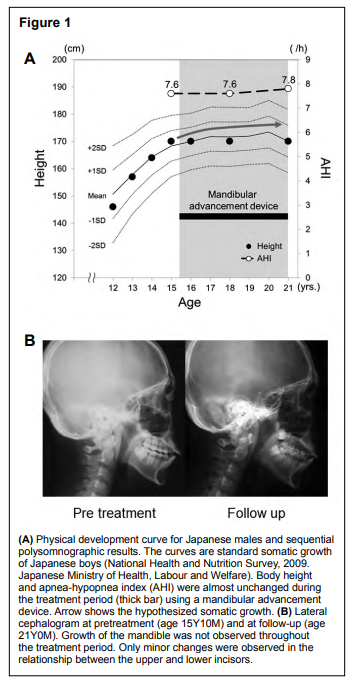
The initial cephalogram revealed that, while the position of the maxilla was normal, the mandible showed both a small size and retroposition in comparison with the Japanese standard values (79.9° for the sella to nasion to subspinal point angle [SNA-- Japanese standard value = 81.4 ± 3.6°], 73.6° for the sella to nasion to supramental point [SNB; 79.6 ± 3.9°], and 6.3° for the subspinal point to nasion to supramental point angle [ANB; 1.8 ± 1.6°]).5,6 According to the physical development curve for Japanese males, his physical growth spurt appeared to be close to being over (Figure 1A). However, we reasoned that the use of an MAD could induce residual growth of the mandible. After a full explanation of the details, including the possible effects of an MAD on mandibular growth and OSA, both the patient and his mother decided to use the device. Written informed consent was obtained from the patient’s mother regarding the anonymous use of the patient’s data for presentation and/or publication.
An adjustable two-piece type MAD was prescribed at an 8 mm ventrally advanced mandibular position. At 2 months after initiation of therapy, the patient became accustomed wearing his MAD for an average of 6 to 7 days/week. A sufficient improvement of AHI was observed with an MAD in place (AHI = 0.8 events/h) after 3 months, when the resolution of snoring and a reduction in daytime sleepiness were confirmed (JESS = 10). However, neither notable growth of the mandible by the 5-year-use of MAD (80.0° of SNA, 72.5° of SNB, and 7.7 of ANB) nor improvement of OSA without an MAD was observed after a 5-year follow-up (AHI = 7.8 events/h) (Figure 1B).
Figure 1 |
{kind=link}
DISCUSSION
Considering the good compliance with device usage in addition to the patient’s cooperation with treatment, we retrospectively concluded that the optimal timing for MAD as an orthodontic intervention had already passed when the patient was introduced to our clinic.Although the concept of using an MAD for orthodontic treatment would be reasonable from the viewpoint of definitive therapy, there appear to be a few barriers that could weaken the feasibility of MAD therapy for a peripubertal OSA patient. First, as in our case, it is still clinically difficult to prospectively consider whether the mandible can really be anticipated to grow further in a pubescent patient, although the physical developmental curve serves as a good reference. Second, the above significant limitation and the knowledge of craniofacial growth/development are, to some extent, specific, and thus unfamiliar to pediatric physicians as well as general dentists, unless they have specialized in sleep medicine.
This report, unlike the report of a similar pubescent OSA case who showed a favorable outcome with an MAD,1 emphasizes the difficulty of MAD treatment as an orthodontic option for pubescent OSA. It is unlikely that this difficulty lies in the specific technique of dental treatment, and instead may be the result of a delayed diagnosis, due perhaps to limited recognition of the characteristic features of craniofacial growth/development. We propose that pediatric physicians and general dentists should consider an orthodontic approach as soon as they encounter pubescent patients with OSA to avoid losing the pertinent window for definitive treatment.
REFERENCES
2. Maeda K, Tsuiki S, Nakata S, Suzuki K, Itoh E, Inoue Y. Craniofacial contribution to residual obstructive sleep apnea after adenotonsillectomy in children: a preliminary study. J Clin Sleep Med 2014;10:973–7.
3. Huynh NT, Desplats E, Almeida FR. Orthodontics treatments for managing obstructive sleep apnea syndrome in children: a systematic review and meta-analysis. Sleep Med Rev 2016;25:84–94.
4. Takegami M, Suzukamo Y, Wakita T, et al. Development of a Japanese version of the Epworth Sleepiness Scale (JESS) based on item response theory. Sleep Med 2009;10:556–65.
5. Nagaoka K, Kuwahara Y. Normal standards for various Roentgen cephalometric and cast model analyses in present day Japanese adults. Part 1. J Jpn Orthod Soc 1993;52:467–80
6. Sakamoto T, Miura F, Iizuka T. Linear Analyses on the developmental changes of dentofacial complex of Japanese by means of roentgenographic cephalometry. J Stomatol Soc Jpn 1963;30:169–82.
ACKNOWLEDGEMENTS
This work was performed at the Institue of Neuropsychiatry, Tokyo, Japan.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication February, 2016
Submitted in final revised form March, 2016
Accepted for publication March, 2016
Address correspondence to: Satoru Tsuiki, Institue of Neuropsychiatry, 1-21-10 Yoyogi, Shibuya-ku, Tokyo, Japan, 151-0033; Tel: +81-3-3374- 9112
DISCLOSURE STATEMENT
This was not an industry supported study. This study was supported by a Grant-in-Aid for Scientific Research (C) from the JSPS [# 25461180] to E. Itoh, by a Grant-in-Aid for Scientific Research (C) from the JSPS [#26463204] to Y. Okawara, by a Grant-in-Aid for Scientific Research (C) from the JSPS [#15K11463] to M. Kobayashi, by a Grant-in-Aid for Scientific Research (C) from the JSPS [#25515009] to Y. Inoue, by a Grant-inAid for Scientific Research (C) from the JSPS [#25515010 and 15H05301] to S. Tsuiki. The authors have indicated no financial conflicts of interest. The sponsors had no role in the design of the study, the collection and analysis of the data, or preparation of the manuscript.
PDF