Case Report 3, Issue 3.1
RPE and Orthodontic Protraction Facemask as an Alternative Therapy for Severe Obstructive Sleep Apnea Associated with Maxillary Hypoplasia
http://dx.doi.org/10.15331/jdsm.5374
Supakit Peanchitlertkajorn, DDS, MDS?
Hayward Braces, Hayward, CA
ABSTRACT
Rapid palatal expander (RPE) and facemask therapy has been used as a treatment for maxillary hypoplasia. When the treatment is performed with an alternate constriction and expansion protocol, a greater degree of maxillary advancement could be achieved. This report demonstrates the treatment as an effective nonsurgical alternative for resolving a severe OSA associated maxillary hypoplasia in a preadolescent patient.
Keywords:
protraction facemask, RPE, OSA, maxillary hypoplasia, orthodontic
Citation:
Peanchitlertkajorn S. RPE and orthodontic protraction facemask as an alternative therapy for severe obstructive sleep apnea associated with maxillary hypoplasia. Journal of Dental Sleep Medicine 2016;3(1):33–34.
INTRODUCTION
Patients with craniofacial abnormalities have a higher prevalence of obstructive sleep apnea (OSA).1 The treatment often focuses on improving an underlying skeletal pattern. A combined rapid palatal expander (RPE) and protraction facemask therapy has been traditionally advocated to treat maxillary hypoplasia.2 The treatment is the most effective when performed in preadolescence.3 An alternate expansion and constriction protocol for RPE/facemask allowed a greater degree of maxillary advancement compared to a conventional technique.4
The expansion of the maxilla with RPE has been shown to resolve OSA in pediatric patients by simultaneously expanding nasal cavity to increase airflow.5 The use of protraction facemask to advance a maxilla was demonstrated to increase a sagittal nasopharyngeal airway.6 However, a combined RPE/ facemask therapy has never been reported to improve OSA symptoms or reduce apnea-hypopnea index (AHI). This case report demonstrates that RPE/protraction facemask therapy with alternate constriction/expansion protocol is an effective treatment for severe OSA associated with maxillary hypoplasia in a preadolescent patient.
REPORT OF CASE
An 8-year-old female Caucasian patient presented with severe OSA with AHI of 51 episodes/hour. She was prescribed CPAP but could not tolerate it. As a result, she did not use CPAP regularly and continued to have clinical symptoms of OSA (witnessed loud snoring, apneic episodes, fatigue, and daytime sleepiness). She was also diagnosed with hypothyroidism, GERD, controlled epilepsy, and seasonal allergy. She has a history of adenoidectomy and tonsillectomy.
The patient presented with class III malocclusion with anterior crossbite and severe anterior crowding in mixed dentition. The palate is high vaulted and narrow (Figure 1). A cephalometric analysis indicated that both maxilla and mandible were hypoplastic (SNA = 74°, SNB = 74°) with Class III skeletal pattern (ANB = 0°). The lateral cephalogram (Figure 1) also showed a constricted sagittal nasopharyngeal space (u-mpaw = 2 mm).
Figure 1Pretreatment intraoral pictures and lateral cephalogram. |
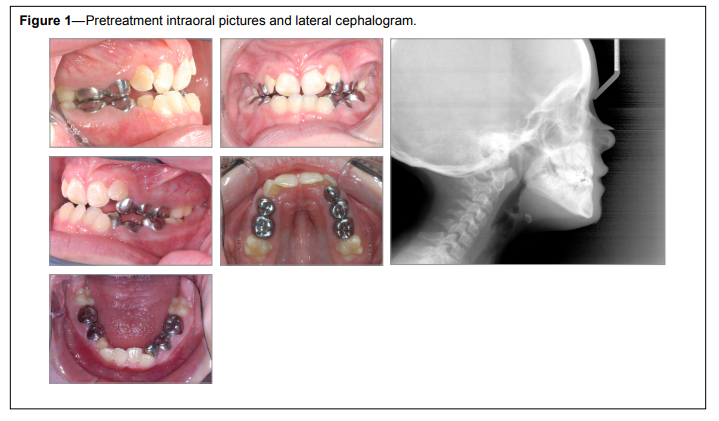{kind=link}
Two treatment options were presented. The first option was to perform a maxillary advancement with distraction osteogenesis. The advancement would significantly increase a nasopharyngeal space and allow for an increased airflow during sleep. This treatment option also requires pre- and post-surgical orthodontic treatment. The second option was a combined use of RPE and protraction facemask with alternate expansion and constriction protocol. In this protocol, the maxilla is expanded, and then constricted, and re-expanded and re-constricted for several cycles before a facemask is applied to start maxillary protraction. This protocol allows for a greater degree of maxillary advancement.4 No surgical procedure is involved in this protocol. The second option was chosen, as it was a less invasive treatment.
After bonding an RPE to upper posterior teeth, parents were instructed to activate the expansion screw 1 turn/day for 7 days. After the initial expansion, the parents were instructed to constrict the palate (1 turn/day) to the original width. The alternate expansion and constriction were repeated for 5 cycles. Following the last cycle, the parents were asked to activate the RPE (1 turn/day) only to expand the palate for 4 weeks. An orthodontic facemask was then delivered after the expansion was completed. The patient was instructed to wear it for 12 h/ day. The patient used RPE and facemask for a period 7 months.
A sleep study performed 15 weeks after starting a facemask therapy showed a significant reduction of AHI to 7 episodes/h with an average oxygen saturation of 97%. No paradoxical breathing was observed during the sleep study. At 17 weeks, the overjet was recorded at 9 millimeters. The patient was then instructed to wear the facemask only a few hours/day to maintain the maxillary position. The RPE and facemask were discontinued after 7 months, as the patient reported a significant improvement of OSA symptoms. A retention device was not considered necessary, as the maxilla was slightly overexpanded. Additionally, RPE was left in place with an adequate amount of time for the maxilla to become stabilized. The post-treatment lateral cephalogram showed a significant increase in both maxillary prominence and nasopharyngeal airway space (SNA = 79°, SNB = 74°, overjet = 8 mm, u-mpaw = 5 mm). The patient underwent another sleep study a month after discontinuation of RPE/facemask. The result showed the AHI was further reduced to 4 episodes/h with average oxygen saturation of 96%.
DISCUSSION
A combined orthopedic effects of maxillary expansion and advancement significantly increased nasopharyngeal space. The increased space subsequently led to AHI reduction and improvement of OSA symptoms for this patient. If OSA symptoms recur, the patient can undergo more invasive treatment options. This is the first case report demonstrating a combined RPE and facemask therapy as an effective alternative for treating a severe OSA associated maxillary hypoplasia.
REFERENCES
2. Kama JD, Ozer T, Baran S. Orthodontic and orthopaedic changes associated with treatment in subjects with Class III malocclusions. Eur J Orthod 2006;28:496–502.
3. Suda N, Ishii-Suzuki M, Hirose K, Hiyama S, Suzuki S, Kuroda T. Effective treatment plan for maxillary protraction: is the bone age useful to determine the treatment plan? Am J Orthod Dentofacial Orthop 2000;118:55–62.
4. Liou EJ. Effective maxillary orthopedic protraction for growing Class III patients: a clinical application simulates distraction osteogenesis. Prog Orthod. 2005;6:154–71.
5. Villa MP, Malagola C, Pagani J, Montesano M, Rizzoli A, Guilleminault C, Ronchetti R. Rapid maxillary expansion in children with obstructive sleep apnea syndrome: 12-month follow-up. Sleep Med 2007;8:128–34.
6. Sayinsu K, Isik F, Arun T. Sagittal airway dimensions following maxillary protraction: a pilot study. Eur J Orthod 2006;28:184–9.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication October, 2015
Submitted in final revised form November, 2015
Accepted for publication November, 2015
Address correspondence to: Supakit Peanchitlertkajorn, DDS, MDS, 1866 B Street, Suite 201, Hayward, CA, 94541; Tel: 510-581-7851; Fax: 510-581-6114; Email: supakit@att.net
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest. The work was performed at the Dallas Children’s Medical Center.
PDF