Case Report 2, Issue 3.1
Lip Muscle Training Improves Halitosis and Obstructive Sleep Apnea Syndrome: A Case Report
http://dx.doi.org/10.15331/jdsm.5372
Mayuko Yoshimiura, DDS1 ; Hiroshi Suzuki, DDS, PhD1 ; Hiroyuki Tanaka, DDS, PhD2 ; Ryuto Asakawa, DDS1 ; Chin-Moi Chow, PhD3 ; Misao Kawara, DDS, PhD1?
Departments of 1 Oral Function and Rehabilitation, and 2Laboratory Medicine for Dentistry, Nihon University School of Dentistry at Matsudo, Chibo, Japan; 3Discipline of Exercise and Sport Science, Faculty of Health Sciences, University of Sydney, Sydney, Australia
ABSTRACT
Halitosis is associated with mouth breathing, dry mouth, snoring, and obstructive sleep apnea syndrome (OSAS). A 40-year-old woman with moderate halitosis showed objective improvement following periodontal treatment for 1 year, but her unpleasant subjective symptoms remained. Lip muscle training using the Patakara trainer (PTR) was implemented to both increase salivary flow and treat her OSAS. After PTR training an increase in lip closure force and a decreased respiratory index (8.2 to 3.2 events/h) were observed. The patient reported resolution of mouth breathing, dry mouth, snoring, and foul odor. PTR training was associated with an improvement in halitosis and respiratory events.
Keywords:
lip muscle training, halitosis, obstructive sleep apnea syndrome, dry mouth
Citation:
Yoshimiura M, Suzuki H, Tanaka H, Asakawa R, Chow CM, Kawara M. Lip muscle training improves halitosis and obstructive sleep apnea syndrome: a case report. Journal of Dental Sleep Medicine 2016;3(1):31–32.
INTRODUCTION
Halitosis results from malodorous substances produced by anaerobic bacteria.1 Standard treatment includes dental cleaning, tooth brushing, mechanical debridement of the tongue, and rinsing with antimicrobial agents.
Salivary flow may be central to the development of halitosis, since saliva has an antimicrobial action, and its slightly acidic pH (6.5) suppresses the growth of Gram-negative and anaerobic bacteria that produce malodorous substances.2 Hence, dry mouth, a side effect of mouth breathing, can lead to halitosis due to reduced salivary flow.1 Mouth breathing also increases upper airway collapsibility3 and the occurrence4 and severity of obstructive sleep apnea syndrome (OSAS) through a narrowed pharyngeal airway.5
A patient with moderate halitosis successfully treated with lip muscle training is presented.
REPORT OF CASE
A 40-year-old woman (BMI 22.1 kg/m2) with no smoking history had a chief complaint of halitosis. She had papillary thyroid cancer and uterine fibroids (both in remission), childhood asthma and allergic rhinitis, and previously took levothyroxine sodium for hypothyroidism. She had no gastroesophageal tract problems.
Malodorous substances (H2S, CH3SH, and (CH3)2S) were analyzed using the Oral Chroma (Abimedical Corp., Osaka, Japan).6 All tests were performed at least 2 hours after a meal, at the same time (10:00 am).
The respiratory disturbance index (RDI) and peripheral oxygen saturation (SpO2) were collected for about 6 hours with the SAS-2100 (Teijin Home Healthcare Limited, Tokyo, Japan) during sleep. Data were downloaded and analyzed using QP-021W software, Ver.01-10 (Nihon Kohden, Tokyo, Japan).
Lip closure force (LCF) was measured with a lip device (BHCV01; Patakara, Tokyo, Japan). The maximum and minimum values obtained in a 10-s period were recorded. LCFmax and LCFmin measurements were repeated three times, and mean values were calculated.
The Lip Muscle Trainer M-Patakara (Patakara Co., Ltd.) for LCF training, made from flexible, resilient plastic, and rubber, is used to increase the strength of the oral muscles. Training (5 min, 4 times/day) was performed for 2 months.5
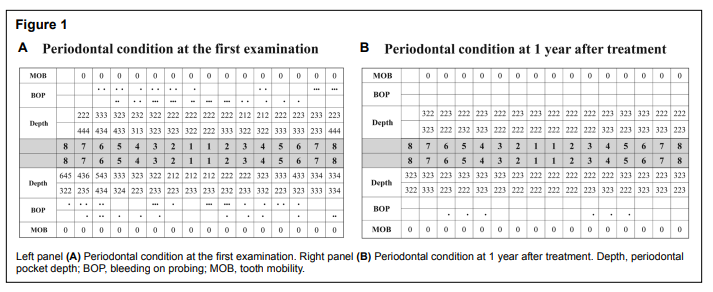
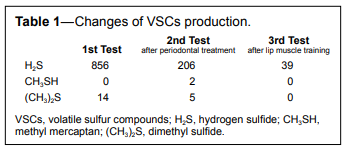
In May 2012, the patient had no caries or missing teeth and no temporomandibular joint (TMJ) abnormalities. Tongue coating area was ≤ 1/3 on the dorsal tongue surface, with no soft tissue problems. She had periodontal pockets ≥ 4 mm in the molar region, and bleeding on probing around most teeth, with no tooth mobility (Figure 1A). H2S was 856 ppb (recognition threshold 112 ppb), CH3SH was 0 ppb, and (CH3)2S was 14 ppb (recognition threshold 8 ppb, Table 1). The patient then received periodontal treatment for halitosis.
Figure 1Pretreatment intraoral pictures and lateral cephalogram. |
{kind=link}
Table 1Changes of VSCs production |
{kind=link}
In July 2013, the patient showed improvement with periodontal pockets ≤ 3 mm around all teeth (Figure 1B). A second halitosis test showed improvement in (CH3)2S from 14 to 5 ppb, and H2S decreased to 206 ppb. (Table 1) However, halitosis remained a concern. Further questioning revealed she suffered from mouth dryness upon awakening and snoring. Her bed partner verified that she snored with her mouth open during sleep. A sleep test confirmed an RDI of 8.2 events/h and minimum SpO2 of 91%, consistent with mild OSAS. A mandibular advancement device (MAD) was then fabricated as a routine treatment for OSAS. A Patakara trainer (PTR) was given to simultaneously treat the coexisting halitosis and OSAS. LCF measurements were taken. The patient discontinued the MAD after several days due to TMJ soreness, and lip muscle training alone was continued.
Two months after starting PTR (November 2013), both maximum and minimum LCF improved, RDI dropped to 3.2 events/h, and the minimum SpO2 increased to 97%. On the third halitosis test, H2S was 39 ppb, below the recognition threshold (112 ppb, Table 1). In June 2014, the patient had continued PTR and showed favorable findings, with no snoring or malodor.
DISCUSSION
The lack of effectiveness of the periodontal approach to halitosis treatment in this case suggested other underlying contributory sources, and further questioning led to the diagnosis of OSAS. After PTR the H2S level was below the recognition threshold, and halitosis was no longer detected. Additionally, RDI dropped and SpO2 improved. These improvements paralleled an increase in LCF, suggesting that PTR strengthened the muscles around the lips and may have caused the decreased RDI and absence of snoring. Furthermore, following PTR training, there was a change from mouth to nose breathing with no snoring during sleep. She no longer experienced dry mouth, perhaps due to increased salivary flow associated with lip muscle training.
In conclusion, lip muscle training was associated with elimination of halitosis and improvement in the RDI and SpO2, likely through increased LCF. A randomized, controlled trial is needed to test the efficacy of lip muscle training in patients with halitosis, OSAS, or coexisting halitosis and OSAS.
REFERENCES
2. Doran A, Kneist S, Verran J. Ecological control: in vitro inhibition of anaerobic bacteria by oral streptococci. Microb Ecol Health Dis 2004;16:23–7.
3. Enoz M. Effects of nasal pathologies on obstructive sleep apnea. Acta Medica (Hradec Kralove) 2007;50:167–70.
4. Lee SH, Choi JH, Shin C, Lee HM, Kwon SY, Lee SH. How does openmouth breathing influence upper airway anatomy? Laryngoscope 2007;117:1102–6.
5. Bachour A, Maasilta P. Mouth breathing compromises adherence to nasal continuous positive airway pressure therapy. Chest 2004;126:1248–54.
6. Oral Chroma instruction manual: measurement procedure and saving measurement data. Osaka Abimedical Corp, 2007.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September, 2015
Submitted in final revised form October, 2015
Accepted for publication November, 2015
Address correspondence to: Hiroshi Suzuki, Department of Oral Function and Rehabilitation, Nihon University School of Dentistry at Matsudo, 870-1 Sakaecho, Nishi-2, Matsudo, Chiba 271-8587, Japan; Tel: +81-47-360-9641; Fax: +81-47-360-9615; Email: suzuki.hiroshi91@ nihon-u.ac.jp
DISCLOSURE STATEMENT
This was not an industry supported study. This study was supported by a Grant-in-Aid for Scientific Research (15K11200) from the Ministry of Education, Culture, Sports, Science and Technology, Japan. The authors have indicated no financial conflicts of interest.
PDF