Case Report 2, Issue 2.1
Effect of Beer Ingestion on a Patient with OSA while Using Oral Appliance Therapy
http://dx.doi.org/10.15331/jdsm.4434
Sheri Katz, DDS
Private Practice, Atlanta, GA
ABSTRACT
It has been shown that alcohol prior to sleep in obstructive sleep apnea (OSA) patients exacerbates the frequency and severity of hypoxic events and shortens the time from sleep onset to the most severe event. Ingestion of a moderate amount of alcohol does not decrease the efficacy of continuous positive airway pressure in treatment of OSA. Oral appliance therapy has been gaining in use as an effective option in the treatment of OSA. The question arises as to whether oral appliance use will protect the patient from the deleterious effects of alcohol ingestion on respiration. In this case report, the OSA patient had ingested alcohol approximately 3 hours before bedtime and then used an overnight oximeter while wearing her oral appliance. She showed significant oxyhemoglobin desaturations soon after retiring for the night. The period of instability lasted for approximately 1.5 hours and was not repeated for the remainder of the night.
Keywords:
oral appliance therapy, alcohol, oxygen saturation
Citation:
Katz S. Effect of beer ingestion on a patient with OSA while using oral appliance therapy. Journal of Dental Sleep Medicine 2015;2(1):17–18.
REPORT OF CASE
A 63-year-old female was referred for complaints of snoring, teeth grinding, acting out dreams, and a morning dry throat. She had a history of dyslipidemia, hypertension, hypothyroidism, and gastroesophageal reflux disease. Her medications included levothyroxine, triamterene, and omeprazole. Her body mass index was 33.2, and her Epworth Sleepiness Scale score was 5/24. The patient had a complete evaluation and polysomnogram which showed respiratory disturbance index (RDI) 22.8, apnea-hypopnea index 15.8, oxyhemoglobin nadir 71%, hypoxic burden of 3.2, supine RDI 22.8, and REM sleep RDI 88.7. Based on these findings, she was diagnosed with moderate obstructive sleep apnea (OSA). The severity of the sleep disordered breathing was significantly worse during REM. She was prescribed continuous positive airway pressure (CPAP) but was told that she would need a full face mask, and felt she would not be able to tolerate it.
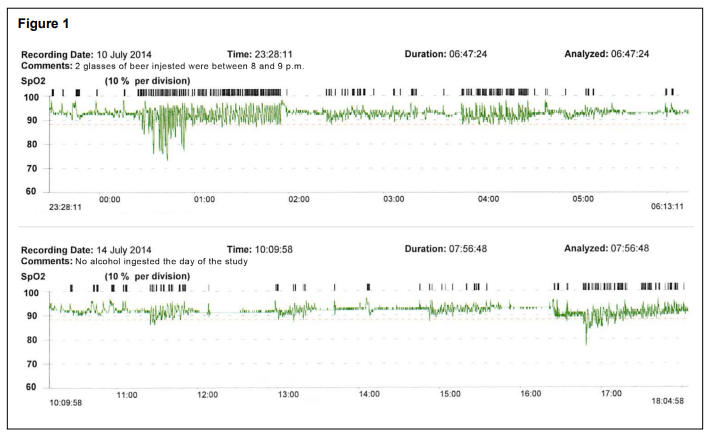
The patient was referred for an evaluation for oral appliance therapy (OAT) for the management of her OSA. The oral evaluation revealed that her tongue level was high, she had a Mallampati III soft palate classification, and her tonsils were grade 1. No other significant abnormalities were noted. These findings were reviewed with the patient and it was agreed that she was a good candidate for OAT. Impressions and records were made, and an oral appliance was fitted and delivered one month later. The patient began using the oral appliance. Appropriate adjustments were made to resolve the patient’s symptoms of snoring, morning headaches, and dry throat. Overnight oximetry was performed with the oral appliance in place. This showed significant oxygen desaturations starting one hour into the study, lasting 1.5 hours (Figure 1). It was noted that the patient had 2 beers between 20:00 and 21:00 on the night of the study. A subsequent study, with no alcohol, was done 1 month later. No such events occurred. The patient is feeling more alert during the day and is not snoring. She has a home sleep study scheduled to validate the efficacy of the oral appliance’s current position.
Figure 1 |
{kind=link}
DISCUSSION
Because these observations were not made by polysomnography, it is not possible to draw definitive conclusions regarding the patients’ awake and sleep time and her sleep stages. However, the most significant desaturations appear to be at the beginning of the night, within the time frame described by Scrima et al., when he described the increase of severity of OSA after alcohol ingestion: “The most severe hypoxic events occurred within 80–160 minutes after sleep onset.”1
Nigri et al.2 and Teschler et al.3 reported that “CPAP can offset the adverse effects of alcohol on the upper airway.” This case study suggested that oral appliance therapy may not be able to offer that same protection. Krol et al. demonstrated that the “neural mechanisms underlying the respiratory activity of the genioglossus are more susceptible to depression by alcohol than those serving the muscles of the ventilatory pump.”4
Further research is warranted to confirm and possibly expand on this observation. If oral appliances are shown to inadequately protect the airway when under the influence of alcohol, patients must be counseled to this effect; CPAP may be a better option for patients that choose to use alcohol regularly.
REFERENCES
2. Nigri DH, Addor G, Franco CA, Martins RC, Gomes MP, Strollo PJ Alcohol induced apnea. J Clin Sleep Med 2005;1:424–6.
3. Teschler H, Berthon-Jones M, Wessendorf T, Meyer HJ, Konietzko N. Influence of moderate alcohol consumption on obstructive sleep apnoea with and without AutoSet nasal CPAP therapy. Eur Respir J 1996;9:2371– 7.
4. Krol RC, Knuth SL, Bartlett D Jr. Selective reduction of genioglossal muscle activity by alcohol in normal human subjects. Am Rev Respir Dis 1984;129:247–50.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication December, 2014 Accepted for publication December, 2014 Address correspondence to: Sheri Katz, DDS, 2172 Lavista Road, Atlanta, GA 30329; Tel: (404) 321-2722; Fax: (404) 343-1845; Email: sherikatz15@ gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Katz has indicated no financial conflicts of interest.
PDF