Case Report 2, Issue 12.1
Myofunctional Therapy as a Combined Treatment to Reduce Occlusal Side Effects of MAD Therapy in OSA Patients: A Clinical Case Report
http://dx.doi.org/10.15331/jdsm.7376
Susana Falardo, DMD, MSC, PhD, IC-ABDSM, BD-EADSM,1 Sandra Marques, MD,2 Amélia Feliciano, MD, PhD3
1Coordinator and Professor of Postgraduation in Sleep Medicine, Catholic Medical School, Portuguese Catholic University, Lisbon, Portugal, Centre for Interdisciplinary Research in Health, Portugal. Orcid: orcid.org/0000-0002-9206-7493; 2 Internal Medicine Physician, Somnologist by European Sleep Research Society, Clinical Director at TRP Sleep Clinic, Lisbon, Portugal; 3Respiratory Physician, Somnologist by European Sleep Research Society, Coordinator of Postgraduation in Sleep Medicine and Associate Professor at Catholic Medical School, Portuguese Catholic University, Lisbon, Portugal.
Abstract:
Obstructive sleep apnea (OSA) syndrome is the most common sleep-disordered breathing disorder and is included in the International Classification of Sleep Disorders, Third Edition sleep-disordered breathing category. The adequate treatment of OSA depends on the severity of symptoms and disease, as well as the anatomic characteristics and the patient's health status. A multidisciplinary approach to the treatment of OSA is mandatory. Although positive airway pressure is the recommended treatment, in some patients a mandibular advancement device (MAD) is beneficial, especially for those with mild to moderate OSA. However, mild and transient adverse effects have been reported in the early stages of therapy. Myofunctional therapy as a combined therapy has shown great results in controlling MAD adverse effects and improving muscle tone.
Case Report:
A selected patient with mild OSA, presenting with diurnal and nocturnal signs and symptoms such as muscular discomfort and temporomandibular joint noises during mouth opening and closing movements, underwent MAD therapy combined with myofunctional therapy using an individualized protocol.
Conclusions:
Myofunctional exercises seem to positively control the adverse effects of MAD by improving muscle tone, reducing muscle discomfort, and stabilizing occlusal contacts. Myofunctional therapy, as a combined treatment, also appears to improve OSA results.
Keywords:
obstructive sleep apnea, MAD, myofunctional therapy, orofacial exercises. morning occlusal guide, occlusal adverse effects.
Citation:
Falardo S, Marques S, Feliciano A. Myofunctional therapy as a combined treatment to reduce occlusal side effects of mad therapy in osa patients: A clinical case report. J Dent Sleep Med. 2025;12(1)
INTRODUCTION
Obstructive sleep apnea (OSA) syndrome is the most common sleep-disordered breathing disorder included in the International Classification of Sleep Disorders, Third edition sleep-disordered breathing category.1 Individuals with OSA experience episodes of partial or complete upper airway obstruction, resulting in sleep fragmentation, hypoventilation, and blood gas abnormalities as hypoxemia.2 Complete or partial collapse of the upper airway can be due to intrinsic or extrinsic factors, such as anatomic, genetic, or neuromuscular factors.2,3 The intrinsic factors are responsible for decreasing the patency of the upper airway, whereas the extrinsic factors, such as fat deposits, tissue hypertrophy, and certain craniofacial features, cause an increase in the external pressure of the upper airway.3,4
The adequate treatment of OSA depends on the severity of symptoms and disease, as well as the anatomic characteristics and the patient´s health status.5 A multidisciplinary treatment approach should be offered for OSA treatment, including ventilation therapy, weight loss, mandibular advancement devices (MADs), and pharyngeal surgery. Nevertheless, the typical treatment for moderate to severe OSA is the use of positive airway pressure overnight.6
Acceptance and therapeutic outcomes with MADs are favorable in many patients, particularly in the treatment of mild to moderate OSA. However, mild and transient adverse effects have been reported during the initial period of therapy. These include dental pain, myofascial pain, temporomandibular joint (TMJ) pain, excessive salivation or dry mouth, and gingival irritation. Long-term use of MADs is associated with changes in craniofacial morphology and dental occlusion, including a reduction in overjet, overbite, and the number of occlusal contact points.5,6
A recent addition to the combined or stand-alone treatment of adult and pediatric OSA is myofunctional therapy (MFT).4,7
MFT aims to balance the tongue muscle tone, soft palate, and face through isometric and isotonic exercises. Also, truthfully the muscle tonus balance by MFT has an important role in controlling TMJ adverse effects and occlusal changes caused by long-term use of the MAD.1,6,7
This relationship stems from the fact that the structures involved in types of sleep-disordered breathing, such as OSA and snoring, are also neuromuscular units, that is, the object of study and intervention with MFT.9
MFT works on the oropharyngeal (soft palate, lateral pharyngeal wall) and oral (lip, tongue) structures. Patients make oral vowel sounds either continuously (isometric exercises) or sporadically (isotonic exercises) as part of soft palate exercises.2,10 Tongue exercises include pressing the entire tongue against the hard and soft palate, moving the tongue along the upper and lateral surfaces of the teeth, and pressing the tongue against the floor of the mouth.2 The tip of the tongue is placed against the anterior aspect of the hard palate.2 Tongue exercises are designed to increase the strength of the tongue's natural movements by increasing muscle tone.9,10
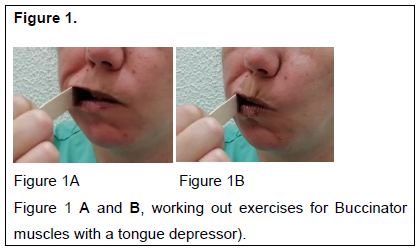
The buccinators exercise includes sucking movements and intraoral finger pressure on the buccinator muscles, the lip contraction and relaxation of the orbicularis, and the jaw muscles (lateral jaw movements) all are targeted by facial exercises.2,10 (Figure 1 A and B, Buccinator exercises with a tongue depressor).
CASE REPORT
Clinical case history
A 29-year-old female patient presented to the clinic with complaints of excessive daytime sleepiness, a score of 16 out of 24 on the Epworth Sleepiness Scale, and a diagnosis of mild OSA.
The diagnostic approach was as follows:
- Anamnesis and history taken by a multidisciplinary sleep team.
- Intraoral/extraoral clinical examination and postural assessment.
- Upper airway examination by an ear, nose, and throat (ENT) specialist and European Sleep Research Society somnologist.
The first diagnostic examination was performed in 2021 and the first posttreatment examination was performed 1 year later in 2022.
Patient examination and clinical observation during the dental visit included the following:
- Diurnal signs and symptoms: Excessive daytime sleepiness; car accident due to sleepiness; memory loss; attention deficit; extreme fatigue; difficulty in completing PhD studies.
- Nocturnal signs and symptoms: Multiple awakenings per night; nocturia; diaphoresis; somniloquy; nightmares and vivid dreams; leg cramps; apnoea and snoring episodes reported by the patient’s bed partner. Other signs and symptoms reported by the patient: no restless sleep; multiple episodes of maintenance insomnia; sleep hygiene disorder; bowel transit complaints suggesting leaky gut.
- Anthropometric and vital assessment of the patient: weight, 48kg; height, 1.68 m; body mass index, 17.0; blood pressure, 127/96 mmHg; diurnal oximetry, 94%; pulse, 62 beats per min; neck circumference, 31 cm.
- Intraoral observation: voluminous tongue, lingual lateral edge edentulism and oral signs of bruxism with posterior tooth wear, traumatic marks on the jugal mucosa, mandibular tori.
- Palpation of the TMJ: Palpation of the left TMJ with crackling during opening and closing movements, without pain or limitation of movement, maximum mouth opening 37 cm.
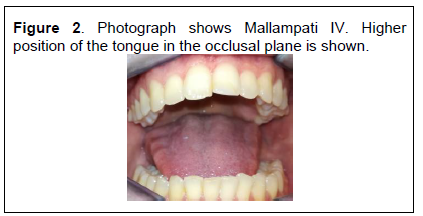
- Mallampati scale type IV.
ENT evaluation
In the ENT clinical assessment, the patient received a diagnosis of rhinosinusitis and was started on medication consisting of ebastine 10 mg, fluticasone furoate spray, 900 mg of diosmin (in micronized form), and 100 mg of flavonoids expressed as hesperidin.
Internal medicine and pulmonologist/somnologist assessment
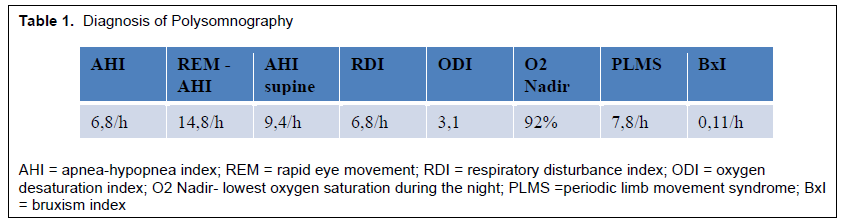
The patient underwent type II ambulatory polysomnography (PSG), using the EMBLETTA MRP PG/ST+PROXY device, recording the following channels: electrocardiogram, electrooculogram, sub Menton and tibial electromyograms, nasal pressure, thermistor, plethysmographic bands (thoracic and abdominal), snoring sensor, oximetry, pulse, and body position. The events analysis was performed manually by different technical specialists and reviewed by a specialist in internal medicine and a European Sleep Research Society somnologist with training and experience in PSG (double scoring) (Table 1).
The PSG study was scored according to the American Academy of Sleep Medicine (AASM) Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications-Version 2.3 2016 Clinical Guidelines for the Evaluation, Management and Long-Term Care of Obstructive Sleep Apnea in Adults, by the American Academy of Sleep Medicine, 2016 edition.
The patient received a diagnosis of mild obstructive respiratory disorder with an apnea-hypopnea index of 6.8 respiratory events/hour, oxygen desaturation index 3.1/hour, and periodic limb movements syndrome 7.8 motors events/hour, and signs of sleep bruxism related to respiratory events scoring bruxism index 0.11/h (Table 1).
PSG also registered signs of multiple nocturnal microarousals. A sleep hygiene disorder was confirmed with the sleep diary and confirmed by actigraphy.
From a clinical point of view, the patient had intestinal transit complaints suggestive of leaky gut, which were under clinical investigation by the internal medicine physician.
Table 1. Diagnosis of Polysomnography |
{kind=link}
Table 2. Polysomnography 3 Months After Mandibular Advancement Device and Myofunctional Therapy |
{kind=link}
Table 3. Polysomnography 9 Months After Mandibular Advancement Device and Myofunctional Therapy |
{kind=link}
Figure 1. |
{kind=link}
Figure 2. Photograph shows Mallampati IV. Higher position of the tongue in the occlusal plane is shown. |
{kind=link}
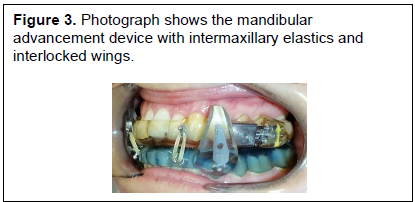
Figure 3. Photograph shows the mandibular advancement device with intermaxillary elastics and interlocked wings. |
{kind=link}
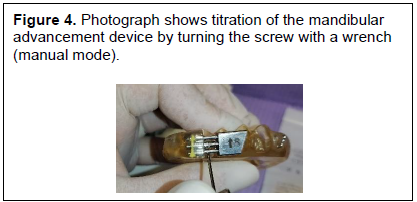
Figure 4. Photograph shows titration of the mandibular advancement device by turning the screw with a wrench (manual mode). |
{kind=link}
{kind=link}
Figure 6. Photograph shows posterior mastication with a silicone morning occlusal guide. |
{kind=link}
Figure 7. Mouth of a patient who underwent myofunctional therapy (MFT). A) Initial presentation. B, After 6 months of MFT C, After 9 months of MFT. |
{kind=link}
DISCUSSION
The patient had no cardiovascular or cerebrovascular pathology, which would have been an indication for positive airway pressure.
Taking into consideration the mild apnea hypopnea index, the bruxism index, and the existence of mild signs and symptoms, an intraoral device therapy was prescribed.
The placement of MAD with interlocking bilateral wings and anterior control of the mouth opening with intermaxillary elastics was performed (Figure 3). The starting position was set at 50% of total range of motion. Although the titration of this MAD consists of turning the screw once a week (Figure 4), no titration was prescribed due to some muscular and TMJ discomfort. A protocol of daily myofunctional exercises was carried out.
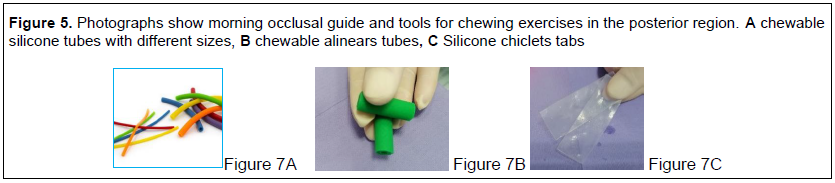
A protocol for daily myofunctional exercises was established, starting with the use of bilateral masticatory exercises (Figure 5) with a morning occlusal guide or a silicone chewing aid the night before adjusting the MAD and the morning after removing the MAD (Figure 6).
The exercises must be performed in a sequence of three series of 10 times on each side in the morning after removal of the mandibular advancement device and, if necessary, in the evening before the mandibular advancement device is adjusted.
Regular orofacial exercises for 10 to 15 minutes per day were also prescribed to increase the muscular tone of the tongue with lingual practice, but also to improve control of the orbicularis of the lip and the buccinator (Figure 1).
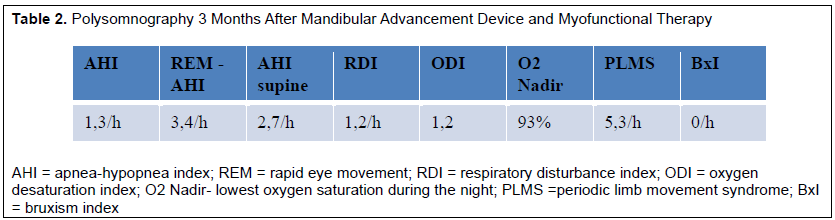
This myofunctional exercise protocol controlled muscular and TMJ discomfort and eliminated the adverse effects of the MAD. After 9 months of MFT, the patient showed improvements in the tongue oropharyngeal position (Figure 7) and on the follow up PSG respiratory events, bruxism, oxygen desaturation index, showed improvements, and also the sleep architecture registers less sleep fragmentation (Table 2). No criteria for the diagnosis of OSA were found on the follow-up PSG. Patients' signs and symptoms resolved and showed improvements in daily quality of life.
CONCLUSION
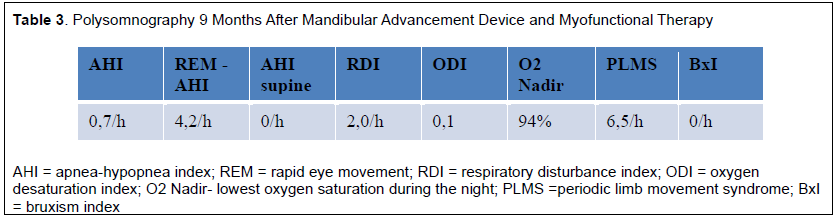
MFT as a combined therapy seems to control muscular response, and TMJ and occlusal MAD adverse effects. An individualized and personalized prescription of exercises is essential to increase muscular tone and balance the orofacial muscular structures. Patients' adherence and compliance also showed improvement in the 9-month follow-up PSG (Table 3).
ABBREVIATIONS
AAMS: American Academy of Sleep Medicine
A/H: Apnoea/Hypopnea
AHI: Apnoea/Hypopnea Index
BxI- Bruxism Index
CPAP- Continue Positive Air Pressure
ECG: Electrocardiogram
EMG: Electromyography
ENT- Otorhinolaryngologist
EOG: Electrooculogram
MAD: Mandibular Advance Device
MFT: Myofunctional Therapy
MOG: Morning Occlusal Guide
NREM: No Rapid Eye Movement
OSA: Obstructive Sleep Apnoea
PLMS: Periodic Limb Movement Syndrome
PSG: Polysomnography
REM: Rapid Eye Movement
UAW: Upper Air Way
REFERENCES
César CPHAR, Sordi C, Baldrighi SEZM, Trench JA, Nascimento GKBO. Respiração oral: intervenção fonoaudiológica e os limites do tratamento – parte I. In: Sordi C, Nahsan FPS, Paranhos LR, organizadores. Coletâneas em saúde. São José dos Pinhais: Editora Plena; 2015. 2v. p. 65-78.
Camacho M, Certal V, Abdullatif J, Zaghi S, Ruoff CM, Capasso R, Kushida CA. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep 2015 May 1;38(5):669-75. doi: 10.5665/sleep.4652.
Kronbauer KF, Trezza PM, Gomes CF. Propostas fonoaudiológicas ao paciente roncador. Distúrb Comun, São Paulo, 25(1): 119-127, abril, 2013. ID: lil-673868.
Torres-Castro R, Vasconcello-Castillo L, Puppo H, et al, Effects of exercise in patients with obstructive sleep apnea. Clocks Sleep. 2021; 3(1): 227-235.
Uniken Venema JAM, Stellingsma C, Doff MHJ, Hoekema A. Dental side effects of long-term obstructive sleep apnea treatment: a comparison of three therapeutic modalities. J Dent Sleep Med. 2018;5(2):39-46.
Attia AAMM, Awad SS, Mansour M, Baz H, Zahran KM, Abdelbaset M. Effects of different treatments for obstructive sleep apnea on temporomandibular joint: a randomized clinical trial. BMC Oral Health.2024;24:931. https://doi.org/10.1186/s12903-024-04623-w.
Ishida E, Kunimatsu R, Medina CC, et al. Dental and occlusal changes during mandibular advancement device therapy in Japanese patients with obstructive sleep apnea: Four years follow-up. J Clin Med.2022; 11:7539 https://doi.org/10.3390/jcm11247539.
O’Connor Reina C, Plaza G, Ignacio-Garcia JM, et al. New Health application software based on myofunctional therapy applied to sleep - disordered breathing in non-compliant subjects. Sleep Science and Practice. 2020;4(3). https://doi.org/10.1186/s41606-019-0040-8.
Sanders I, Mu L, A three - dimensional atlas of the human tongue muscles. Anat Rec (Hoboken). 2013; 296:1102–1114.
Kushida CA, Guimarães KC Drager LF, Genta PR, Marcondes BF, Lorenzi-Filho G. Effects of Oropharyngeal Exercises on Patients with Moderate Obstructive Sleep Apnea Syndrome. Am J Respir Care Crit Care Med. 2009;179(10:962–966.doi:10.1164/rccm.200806-981OC.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted November 18, 2024
Accepted for publication December 9, 2024
Address correspondence to: Susana Falardo, DMD, MSC, PhD, IC-ABDSM, BD-EADSM. Email: susana.falardo@gmail.com.
DISCLOSURE STATEMENT
The authors report no conflicts of interest.
PDF