Case Report 2, Issue 11.3
Case Report: Multidisciplinary Treatment of Obstructive Sleep Apnea and Dental Malocclusion
http://dx.doi.org/10.15331/jdsm.7348Maria Sokolina, DDS, D.ABDSM
1 Harmony Dental Arts, Clifton, NJ
ABSTRACT
When addressing obstructive sleep apnea (OSA) in patients, it becomes crucial to consider additional dental factors such as dental malocclusions and bruxism. Taking a personalized approach that takes into account individual anatomy, medical history, lifestyle, and preferences is vital for comprehensive patient care. In this report, we present a case study where a combination of oral appliance therapy, clear aligners, myofunctional therapy, and home remedies for nasal congestion provided remarkable enhancements in the patient's sleep quality and breathing patterns. This case underscores the importance of employing a multidisciplinary strategy when managing OSA patients with concurrent dental conditions, highlighting the significance of integrating various treatment modalities for optimal outcomes.
Keywords:
Obstructive sleep apnea (OSA),Misaligned teeth, Orthodontic treatment, CPAP therapy, Aligner Sleep Appliance (ASA), Clear aligners, Phenotyping, Sleep apnea treatment, Restorative goals, Multidisciplinary approach, Myofunctional therapy, Nasal
saline irrig
Citation:
Sokolina M. Case report: Multidisciplinary treatment of obstructive sleep apnea and dental malocclusion. J Dent Sleep Med. 2024;11(3)
INTRODUCTION
Obstructive sleep apnea (OSA) affects 2% to 4% of middle-aged Americans, with up to 25% of men aged 30 to 49 years potentially experiencing sleep-disordered breathing.1-3 Continuous positive airway pressure (CPAP) therapy is the gold standard treatment for OSA, but many patients are unable to comply with this treatment. Mandibular advancement devices are a common alternative for patients who do not tolerate or prefer not to use CPAP therapy.4 However, many patients with OSA have coexisting dental pathologies such as dental malocclusion,5 teeth crowding, and significant loss of tooth structure due to wear. These conditions can complicate OSA treatment and can also require treatment to decrease OSA severity.6
CASE REPORT
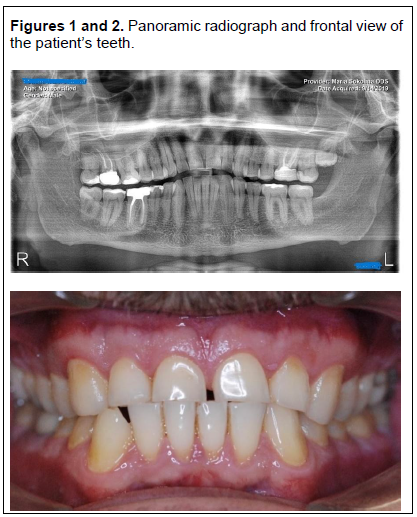
A 47-year-old male with moderate sleep apnea and CPAP intolerance was referred to our practice. The patient reported claustrophobia, difficulty turning the body with the CPAP machine on, and removing the mask during sleep. He also had nasal congestion and complained of waking up with a dry mouth, with or without a CPAP machine. His primary issue was feeling tired and fatigued upon waking. Upon oral examination, the patient's tongue exhibited low muscle tone and scalloping, making it difficult to maintain suction on the palate. Dental examination revealed upper uneven spacing, lower dental crowding, and substantial loss of tooth structure due to attrition. The patient had an edge-to-edge anterior relationship (Figure 1 and 2) with a loss of tooth structure on teeth numbers 7, 8, 9, and 10, leading to a loss of anterior guidance and balancing contacts bilaterally. The initial home sleep study results showed an apnea-hypopnea index (AHI) of 19 events/h, a supine AHI of 30 events/h, a respiratory disturbance index of 19, a nadir oxygen level of 84, and an oxygen desaturation index of 19.
TREATMENT PLAN
The patient was offered two treatment options. The first option involved using a dorsal oral appliance to protrude the lower jaw and tongue forward, increasing the airway dimensions. However, this solution only addressed the patient's breathing problems, leaving the underlying dental pathology intact. The more comprehensive treatment plan involved several steps:
- Myofunctional Therapy: The patient was referred to a myofunctional therapist to address issues with the tongue's tone and function, promote nasal breathing, and create lip competency.
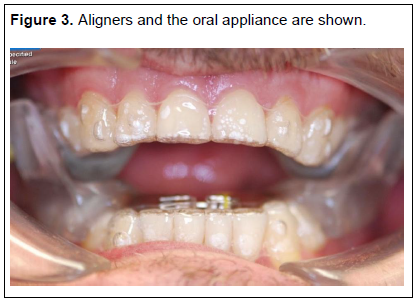
- Clear Aligner Therapy: Clear aligner therapy (Invisalign) in combination with the Aligner Sleep Appliance® (ASA; SleepArchiTx, Newport Beach, CA) was used to correct crowding and expand the arch horizontal dimensions while treating OSA.7 The ASA assisted in both dental arch expansion and protruding the lower jaw and tongue forward at night, ultimately increasing the airway's dimensions (Figure 3).
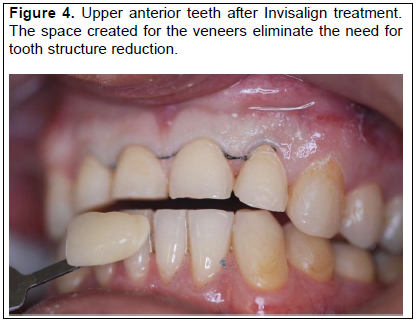
- Restorative Treatment: To restore the tooth structure lost due to malocclusion and wear, no-preparation zirconia veneers were recommended. The patient expressed concerns about reducing tooth structure for veneer preparation and possible sensitivity. To address these concerns, it was ensured that there was enough space between the upper and lower anterior teeth, as well as interproximal spaces between teeth numbers 7, 8, 9, and 10, to enable the placement of the veneers without any tooth reduction and minimize the risk of post operative sensitivity (Figure 4).
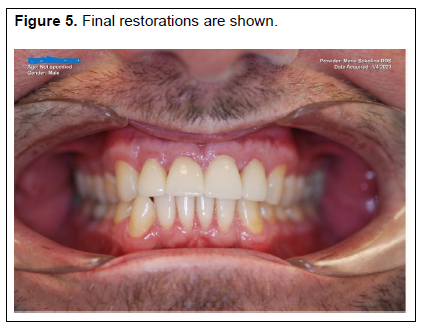
The patient was instructed to wear custom clear aligners for 20 to 22 hours a day and the ASA every night on top of the clear aligners. The patient was provided with 13 aligners for the upper arch and 15 aligners for the lower arch. The ASA had a 5-mm expansion screw to accommodate the expansion with clear aligners. When the patient changed to the next clear aligner, there were issues with the retention of the ASA. To address this, the patient was advised to place the ASA appliance in hot water to soften the internal lining and make it more pliable. The patient found relief from nighttime nasal congestion by using saline nose rinses but was hesitant to try taping his lips at night. To promote nasal breathing and prevent mouth breathing during sleep, the patient was advised to gradually integrate lip taping into their routine, starting with short periods during the day and gradually increasing the duration. Lip taping is thought to help alleviate dryness in the mouth by encouraging nasal breathing.8 The patient had no issues adjusting to the combination therapy of clear aligners and ASA. Initially, he experienced increased salivation and slight discomfort, which were addressed in a follow-up call. The ASA was gradually expanded two turns with every new aligner and reached a maximum of 5 mm of expansion by the end of the treatment with clear aligner. The patient reported reduced snoring and improved sleepiness and fatigue based on the Epworth Sleepiness and Fatigue Scales and SnoreLab app. A follow-up sleep study showed improvements in multiple measures of OSA severity. The patient received zirconia veneers on teeth numbers 7 through 10 after completing active aligner therapy (Figure 5).
The retention of the ASA and clear aligners was suboptimal after orthodontic and restorative treatment, and the patient was given two options: to use clear aligner retainers with ASA or to order a new Respire Blue Oral appliance (Whole You Dental Laboratory, Brooklyn, New York, USA). He chose to use the Respire Blue oral appliance for nighttime wear and clear aligner retainers during the day for 2 hours for 1 year.
The patient has been tested for OSA after the combination treatment. The final home sleep study results showed an apnea-hypopnea index (AHI) of 4 events/h (vs 19 events/h), a supine AHI of 6 events/h (vs 30 events/h), a respiratory disturbance index of 4 (vs 19), a nadir oxygen level of 89 (vs 84), and an oxygen desaturation index of 4 (vs 19).
The patient was placed on a recall schedule in accordance with the guidelines of the American Academy of Dental Sleep Medicine,9 with appointments scheduled every 6 months for the first year and once a year thereafter. The patient was advised to see his sleep doctor annually for evaluation.
Figures 1 and 2Panoramic radiograph and frontal view of the patient’s teeth. |
{kind=link}
Figure 3Aligners and the oral appliance are shown. |
{kind=link}
Figure 4Upper anterior teeth after Invisalign treatment. The space created for the veneers eliminate the need for tooth structure reduction. |
{kind=link}
Figure 5Final restorations are shown. |
{kind=link}
DISCUSSION
This case exemplifies a complex patient scenario that necessitated a multidisciplinary treatment approach. The patient's condition required concurrent management of OSA and dental edge-to-edge malocclusion. The combination of clear aligners with the ASA concurrently corrected the edge-to-edge malocclusion and alleviated the preexisting OSA. Consequently, the patient's OSA substantially improved, as evidenced by the decrease in both the AHI and supine AHI from moderate to severe levels to clinically minimal. Although combining oral appliance therapy with orthodontic and restorative treatment can be controversial, the use of clear aligners along with the ASA can address tooth misalignment, achieve restorative goals, and offer a solution to patients with OSA who have crowded, misaligned teeth that obstruct tongue space and force the tongue into the airway. This approach has the potential to provide a beneficial solution for practitioners preparing their patients for orthognathic surgery to correct OSA and who do not consider CPAP as a temporary option.
CONCLUSION
When treating patients with OSA, it is crucial to consider coexisting dental conditions, such as significant loss of tooth structure due to attrition and dental malocclusions.5,6 Customized treatment plans that address individual anatomy, medical history, lifestyle, and preferences are indispensable for comprehensive care. This case study illustrates how a combination of oral appliance therapy, clear aligners, myofunctional therapy, and home remedies to relieve nasal congestion substantially improved the patient's sleep and breathing quality. This underscores the importance of a multidisciplinary approach when treating patients with OSA who have dental conditions. This approach signifies a significant advancement in the field of dental sleep medicine by providing a comprehensive and customized treatment plan for patients with complex dental sleep conditions.
REFERENCES
- Balasubramaniam R, Klasser GD, Cistulli PA, Lavigne GJ. The link between sleep bruxism, sleep disordered breathing and temporomandibular disorders: An evidence-based review. J Dent Sleep Med. 2014;1(1):27–37.
- Cohen-Levy J, Quintal MC, Rompré P, Almeida F, Huynh N. Prevalence of malocclusions and oral dysfunctions in children with persistent sleep-disordered breathing after adenotonsillectomy in the long term. J Clin Sleep Med. 2020;16(8):1357-1368. doi: 10.5664/jcsm.8534. PMID: 32356517; PMCID: PMC7446101.
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230-1235. doi:10.1056/NEJM199304293281704
- Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc Am Thorac Soc . 2008;5(2):173-178. doi:10.1513/pats.200708-119MG
- Leck R, Paul N, Rolland S, Birnie D. The consequences of living with a severe malocclusion: A review of the literature. J Orthod. 2022 ;49(2):228-239. doi:10.1177/14653125211042891. Epub 2021 Sep 6. PMID: 34488471; PMCID: PMC9160782.
- Kandasamy S, Goonewardene M. Class II malocclusion and sleep-disordered breathing. Semin Orthod . 2014;20(4):316-323. doi:10.1053/j.sodo.2014.09.007
- Ataii P. Performing orthodontics while treating OSA. Inside Dentistry. 2019;15(2). Accessed April 21, 2024.
- Lee Y-C, Lu C-T, Cheng W-N, Li H-Y. The impact of mouth-taping in mouth-breathers with mild obstructive sleep apnea: A preliminary study. Healthcare (Basel). 2022;10(9):1755. Published online 2022 Sep 13. doi: 10.3390/healthcare10091755 PMCID: PMC9498537 PMID: 36141367
- Ramar K, Dort LC, Katz SG, et al. Clinical Practice Guideline for the Treatment of Obstructive Sleep Apnea and Snoring with Oral Appliance Therapy: An Update for 2015: An American Academy of Sleep Medicine and American Academy of Dental Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2015;11(07):773-827. doi:10.5664/jcsm.4858
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication May 25, 2023
Submitted in final revised form December 12, 2023
Accepted for publication June 6, 2024
Address correspondence to: Dr. Maria Sokolina, DDS, D.ABDSM; Email: msokolina94@gmail.co