Case Report 2, Issue 1.1
Oral Appliance Treatment in a Patient with Down Syndrome
http://dx.doi.org/10.15331/jdsm.3734
B. Gail Demko, DMD, D. ABDSM
Sleep Apnea Dentists of New England, Weston, MA; President, American Academy of Dental Sleep Medicine
Treatment of patients with physical and mental disabilities is one of the more difficult undertakings in dental sleep medicine. Most patients have minimal physical difficulty placing, removing, and adjusting their oral appliance (OA). They understand the instructions that are given and comprehend the possibilities of side effects. Patients with Down syndrome, mild dementia, and those with physical limitations such as cerebral palsy and status post cerebral-vascular accident may find OA therapy extremely challenging. Many of these patients have already failed positive airway pressure (PAP) and are sent to a sleep dentist for “salvage therapy.” While presenting challenges to the dental sleep medicine clinician, many of them can become happy and compliant patients.
Over 50% of persons with Down syndrome suffer from obstructive sleep apnea secondary to mid-face deficiency and macroglossia.1-3
A high-functioning 26-year-old male with Down syndrome presented with a history of loud snoring and falling asleep whenever he was a passenger in the car. He had undergone evaluation by an otolaryngologist who found no nasal abnormality and felt that soft tissue surgery was not indicated. The patient had also been evaluated by a maxillofacial surgeon, but the parents had decided not to proceed with surgical treatment. The patient had been on PAP using a number of different interfaces but always developed aerophagia and the pain resulted in his removing the CPAP apparatus within one hour.
The patient lives at home with his mother and stepfather. He works during the day in a protected workshop and tends to stay active by taking karate lessons. His normal bedtime is ~10:00 PM, and his sleep latency is anywhere from 10–60 min. His preferred sleep position is supine. He has a minimally restored 28-tooth dentition with an overjet of 0 mm and an overbite of 0 mm; his range of motion is +6 mm–0 mm.
The overall goal of treatment was to provide increased interincisal distance and mild advancement to allow the macroglossic tongue to move forward out of the upper airway.4 Particular concerns with this patient were his ability to place and remove the oral device without assistance, his limited range of mandibular motion, and a negative reaction to previous therapy.
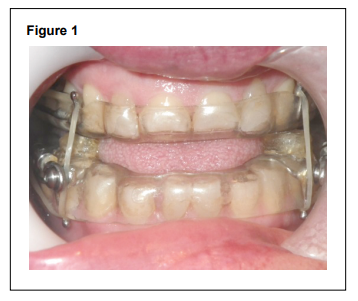
Because the patient was relatively averse to the tight-fitting straps with PAP, it was decided not to use any device that required heating under hot water prior to placement or was laminated for a very tight retentive fit. A hard acrylic device that could be made relatively loose, easy to place, and allow relatively free mandibular movement was chosen as most likely to be tolerated by the patient. A hard acrylic Herbst device with no elastics was fabricated. The bite registration was made using a Pro gauge with a 10-mm interincisal bite fork in the hopes of creating increased tongue space. Additional tongue space was developed by keeping the interocclusal acrylic out of contact in the second molar area; the only contact was in the bicuspid—first molar area. At placement, his tongue naturally moved forward into the resulting interincisal space (Figure 1).
Figure 1 |
{kind=link}
At follow-up, his stepfather reported that the patient sleeps much better with the OA in place and wakens more refreshed. His attitude is more positive and he is less prone to sullen behavior and decreased communication. Both parents were extremely happy with therapeutic outcomes. This patient has not yet been back to see his sleep physician for follow-up polysomnography.
Treatment of patients with disabilities can be very rewarding. One must remember that device choice must be dictated by physical limitations both of oral anatomy and eye-hand coordination. There are number of devices presently on the market which can be easily used for this segment of our population who can be well served with an oral device.
CITATION
Demko BG. Oral appliance treatment in a patient with down syndrome. Journal of Dental Sleep Medicine 2014;1(1):25–26.REFERENCES
2. Churchill SS, Kieckhefer GM, Landis CA, Ward TM. Sleep measurement and monitoring in children with Down syndrome: a review of the literature, 1960-2010. Sleep Med Rev 2012;16:477-88.
3. de Miguel-Diez J, Villa-Asensi JR, Alvarez-Sala JL. Prevalence of sleepdisordered breathing in children with Down syndrome: polygraphic findings in 108 children. Sleep 2003;26:1006-9.
4. Yoshida K. Elastic retracted oral appliance to treat sleep apnea in mentally impaired patients and patients with neuromuscular disabilities. J Prosthet Dent 1999;81:196-201.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication January, 2014
Accepted for publication January, 2014
Address correspondence to: B. Gail Demko, DMD, 140 Merriam St., Weston, MA 02493; Tel: (617) 964-4028; Fax: (617) 595-4591; E-mail: DrDemko@SleepApneaDentist.com
DISCLOSURE STATEMENT
This was not an industry supported study. The author has indicated no financial conflicts of interest.
PDF