Case Report 1, Issue 7.2
Temporomandibular Disorders as an Adverse Effect of Oral Appliance Therapy for the Management of Obstructive Sleep Apnea: A Case Report
http://dx.doi.org/10.15331/jdsm.7122
Sripriya Jayaraman, DDS, MPH1; Jeffrey P. Okeson, DMD2; Isabel Moreno-Hay, DDS, PhD3
1Resident, Orofacial Pain Center, College of Dentistry, University of Kentucky; 2Professor and Interim Dean, College of Dentistry, University of Kentucky; 3Assistant Professor, Program Director, and Interim Division Chief, Orofacial Pain Center, College of Dentistry, University of Kentucky
ABSTRACT
Positive airway pressure therapy is the most common method of management for snoring and obstructive sleep apnea (OSA). However, oral appliance therapy (OAT) has proved to be an effective alternative because of a poor rate of patient adherence, especially in primary snoring and mild to moderate cases of OSA.1,2 Nevertheless, OAT is not exempt from adverse effects, which may include excessive salivation, dry mouth, dental sensitivity, mucosal irritation, occlusal changes, and development or worsening of signs and symptoms of temporomandibular disorders (TMD).2 Furthermore, the development of these adverse effects may compromise the success of OAT for the management of OSA. This case report highlights the importance of early management of signs and symptoms of TMD after initiation of OAT to minimize the risk for discontinuation of therapy with an oral appliance for the management of OSA.
Keywords:
TMD, temporomandibular joint disorders, mandibular advancement device, MAD, oral appliance therapy, OAT, pain
Citation:
Jayaraman S, Okeson JP, Moreno-Hay I. Temporomandibular Disorders as an Adverse Effect of Oral Appliance Therapy for the Management of Obstructive Sleep Apnea: A Case Report. J Dent Sleep Med. 2020;7(2)
INTRODUCTION
The prevalence of obstructive sleep apnea (OSA) is estimated to be 4% in middle-aged men and 2% in middle-aged women.3 Mandibular advancement devices (MAD) can be used effectively in the management of OSA because they prevent the collapsibility of the upper airway by protruding the mandible.2,4 Consequently, a potential adverse effect of these devices is transient pain in the masticatory system, particularly, in patients with previous signs and symptoms of temporomandibular disorder (TMD).2,4,5 In some patients, the pain may be severe enough that oral appliance therapy (OAT) would be abandoned. Thus, proper early management of TMD is crucial for the success of OAT.
TMD is defined as a collective term that encompasses “a number of clinical problems that involve the masticatory muscles, the temporomandibular joints (TMJ), or both.”6 The prevalence of TMD has been reported to be approximately 10% to 15% in the general adult population, and it is almost twice as common in women than in men.7 The etiology of TMD has proved to be multifactorial and many risk factors have been associated with the development and the perpetuation of TMD. Etiologic factors that have been associated with TMD include trauma, anatomic factors, systemic and local pathophysiologic factors, genetic factors, and psychosocial factors.6 However, there is limited evidence in the literature about the incidence of TMD in patients with OSA treated with OAT. Moreover, further studies are needed on the management of adverse effects related to the use of MAD to minimize the failure of OAT.
REPORT OF CASE
A 61-year-old woman was referred by her sleep physician for management of mild OSA with OAT. She had undergone polysomnography (PSG) at a sleep center and the results were reviewed and interpreted by a board-certified sleep physician, revealing an apnea-hypopnea index of 9.9 events per hour and minimum oxygen saturation of 88%. The patient reported mild snoring, witnessed apneas, daytime tiredness, and poor sleep quality. Her Epworth Sleepiness Scale score was 5. Reportedly, she had a trial of continuous positive airway pressure therapy but was unable to tolerate it. She also reported a history of right TMJ popping sounds present for many years that occasionally (three to four times a month) were associated with mild pain (3/10 in intensity) triggered by chewing hard foods and opening her mouth wide.
Her medical history was positive for diabetes, hypertension, and gastroesophageal reflux disease. At her initial consultation, her weight was 209 lb with a body mass index of 33.7 kg/m2 and neck circumference of 17.5 inches. Mallampati classification was class IV. Palpation of the masticatory structures revealed bilateral tenderness of temporal tendons and tenderness of the right TMJ capsule. A repeatable opening click was noted on the right TMJ. Maximum mouth opening was 48 mm with deviation to the right, overbite 3 mm, overjet 3 mm, right excursive 6 mm, left excursive 9 mm, and protrusive of 10 mm. A panoramic radiograph was obtained before initiating treatment. The image showed bilateral, rounded, well-corticated TMJ condyles. Her dentition appeared well restored with good periodontal support. A 5-mm George gauge was used to record her protrusive. Her vertical dimension was checked at the time of bite registration and appliance delivery. A Herbst MAD was delivered at 50% of maximum protrusive movement.
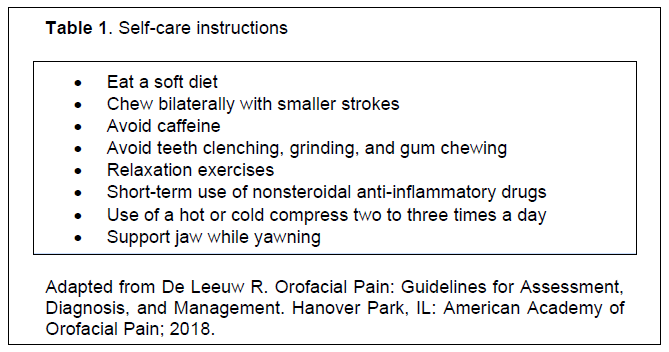
At 2-week follow-up, the patient reported pain that began 1 week after initiation of the treatment and located bilaterally in the preauricular area with an intensity of 6/10 upon awakening and during meals. Clinical examination revealed pain on palpation of bilateral masseter muscles, temporal tendons, and TMJs, which was consistent with a diagnosis of masticatory myalgia and bilateral TMJ arthralgia secondary to the use of the MAD, according to the diagnostic criteria for temporomandibular disorders. Along with continued use of the MAD during sleep, conservative treatment was recommended including soft diet, application of warm compress for 10 to 15 minutes 2 to 3 times a day, clenching awareness, habit reversal, and clock-regulated ibuprofen 400 mg three times a day for 2 weeks. However, despite the initial conservative approach (Table 1), the pain escalated to an intensity of 9/10 and OAT was temporarily discontinued. The patient resumed the continuous positive airway pressure therapy and continued the conservative management of TMD4 for approximately 2 months until symptoms improved. MAD was then reintroduced at 2 mm of advancement (20% of maximum protrusion instead of 50%) in addition to self-care strategies. At 1-month follow-up the patient reported a significant improvement of symptoms (visual analog scale score = 2/10) and good tolerance of the MAD. Titration of the appliance was then initiated by small increments of 0.5 mm every month. At 6- month follow-up, the patient had been wearing her appliance every night and reported complete resolution of her pain complaints in addition to an 80% improvement in sleep quality. She was referred back to her physician for a second sleep study with the appliance in place.
Table 1Self-care instructions |
{kind=link}
DISCUSSION
TMD can be a transient adverse effect associated with the use of MADs, particularly during the initial phases of treatment.2 Therefore, patients with prior signs and symptoms of TMD may experience an exacerbation of those symptoms. Patients with OSA should be screened for TMD prior to the initiation of OAT and during the subsequent follow-up appointments, so early detection and management of TMD can be implemented to prevent the discontinuation of OAT because of adverse effects.
REFERENCES
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015; 11(7):773–827.
- Perez C, De Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2013;17(1):323–332
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230-1235.
- Martınez-Gomis J, Willaert S, Nogues L, Pascual M, Somoza M, Monasterio C. Five years of sleep apnea treatment with a mandibular advancement device. Side effects and technical complications. Angle Orthod, 2010;80(1):30-36.
- Sheats RD, Schell TG, Blanton AO, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;4(4):111–125.
- De Leeuw R. Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management. Hanover Park, IL: American Academy of Orofacial Pain; 2018.
- List T, Højland Jensen R. Temporomandibular disorders: Old ideas and new concepts. Cephalalgia. 2017;37(7):692–704.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication August 19, 2019
Submitted in final revised form December 5, 2019
Accepted for publication December 13, 2019
Address correspondence to: Sripriya Jayaraman, DDS, MPH, Orofacial Pain Center, Kentucky Clinic E 214, 740 South Limestone , Lexington, KY- 40536; Email: sja288@uky.edu.