Case Report 1, Issue 3.2
Maxillomandibular Advancement Surgery as a Treatment of Obstructive Sleep Apnea in a Patient with Cleidocranial Dysostosis: A Case Report
http://dx.doi.org/10.15331/jdsm.5722
Heather Chance, DMD; Lee Pollan, DMD, MS
Oral and Maxillofacial Surgery, University of Rochester, Rochester, NY
ABSTRACT
Study Objectives:
Maxillomandibular advancement surgery is a well-supported treatment option for obstructive sleep apnea in patients who have not responded to or who have not tolerated nonsurgical management. The usual straightforward surgical procedure can be made much more difficult with numerous impacted supernumerary teeth, as is frequently seen in patients with cleidocranial dysostosis.
Methods:
The preoperative planning, surgical procedure, and postoperative phase of the maxillomandibular advancement surgery for a 51-year-old patient with severe OSA (apnea-hypopnea index 94 events/h in 2010) and concomitant cleidocranial dysotosis will be discussed in this case report.Results:
When compared to the preoperative polysomnographic examination, striking improvements were noted on the examination at 8 months after surgery (apnea-hypopnea index from 94 to 21 events/h).Conclusions:
The results of this case showed that using traditional maxillomandibular advancement surgical protocols, despite the numerous impacted supernumerary teeth, provides excellent results for the treatment of severe OSA. The patient will require further follow-up and likely subsequent treatment of his remaining dentition.Keywords:
obstructive sleep apnea, cleidocranial dysplasia, telegnathic surgery, maxillomandibular surgery
Citation:
Chance H, Pollan L. Maxillomandibular advancement surgery as a treatment of obstructive sleep apnea in a patient with cleidocranial dysostosis: a case report. Journal of Dental Sleep Medicine 2016;3(2):65–70.
INTRODUCTION
Obstructive sleep apnea (OSA) is characterized by intermittent but prolonged upper airway obstruction that disrupts normal ventilation during sleep.1 It is often associated with daytime somnolence, neurocognitive deficits, and an increased risk of cardiovascular events which leads to overall increased morbidity and mortality.2 The American Academy of Sleep Medicine classifies severity of OSAS based on the mean number of apneas and hypopneas per hour during sleep (AHI).3 Mild between 5 and 15, moderate 15–30, and severe greater than 30.4
Cleidocranial dysostosis is an autosomal dominant congenital defect that involves the development of the teeth and bones. It is thought to involve the RUNX2 gene which is responsible for making a protein involved in cartilage and bone development and maintenance.5 Without the functioning gene, individuals with cleidocranial dysotosis may have osteopenia, underdeveloped or absent clavicles, delayed closure of the fontanels, and short stature. In terms of the facial skeleton, brachycephaly, frontal bossing, and hypertelorism are common. Dental abnormalities including delayed exfoliation of primary teeth, delayed eruption of the permanent dentition, malformed teeth, malocclusion, and multiple supernumerary teeth. In addition, may patients with cleidocranial dysotosis present with hearing loss and increased incidence of ear and sinus infections.6
There is no current evidence to suggest a link between OSA and cleidocranial dysostosis and the treatment of a patient with both may present a challenge to the treating surgeon. With the typical presentation of multiple impacted supernumerary teeth, both the actual maxillomandibular advancement surgical osteotomies and fixation have the potential to be much more difficult.
REPORT OF CASE
A 51-year-old man with known cleidocranial dysostosis and obstructive sleep apnea presented to the University of Rochester, Strong Memorial Hospital Oral and Maxillofacial Surgery clinic for surgical evaluation. He was diagnosed with extremely severe OSA 7 years earlier (2006), with a polysomnographic examination that showed an apnea-hypopnea index (AHI) = 84 episodes/h; time of sleep with SpO2 < 90% = 17 min (5%); total sleep time (TST) = 347 min. At that point, he was treated with a CPAP that he was, unfortunately, unable to tolerate. He had a second polysomnographic examination in 2010 which again revealed extremely severe OSA with an (AHI) = 94 episodes/h; time of sleep with SpO2 < 90% = 135 min (49.8%); total sleep time (TST) = 313 min. The patient reported multiple episodes of falling asleep while driving and has had several minor motor vehicle accidents as a result. He has a past medical history significant for mild GERD, controlled hypertension, angina pectoris, and congestive heart failure (ejection fraction = 35%). He reported an untreated depression and felt that his constant feeling of fatigue was related.
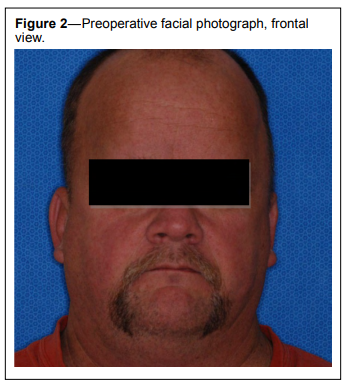
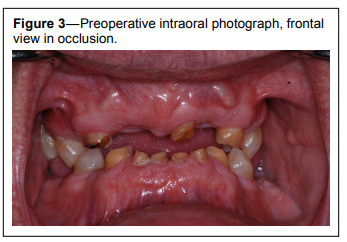
The general physical examination revealed a well-nourished, well developed patient with a BMI on initial presentation of 37.9. He was, at that time, enrolled in a weight loss program. He presented with a flat profile, frontal bossing, and sunken nasal bridge. He had some degree of hearing loss bilaterally, present since birth. He had no nasal or sinus complaints, no soft palate, tonsillar, or tongue base hypertrophy though he did present with a Mallampati III airway with a maximum incisal opening of approximately 28 mm (Figures 1 and 2). He had multiple palpable and multiple non-palpable impacted teeth. The only erupted teeth present intraorally were teeth numbers 4, 5, 12, 21, 28, and primary teeth C, F, H, M, N, O, P, Q, R therefore there was no measurable occlusion (Figure 3).
Figure 1Preoperative facial photograph, lateral view. |
{kind=link}
Figure 2Preoperative facial photograph, frontal view. |
{kind=link}
Figure 3Preoperative intraoral photograph, frontal view in occlusion. |
{kind=link}
A panoramic radiograph (Figure 4) revealed fully impacted teeth #1, 2, 6, 7, 8, 9, 10, 11, 15, 16, 17, 18, 19, 22, 23, 24, 25, 26, 27, and 32. The ascending ramus are slightly narrow and the coronoid processes thin and pointed.
Figure 4Preoperative orthopantogram radiograph. |
{kind=link}
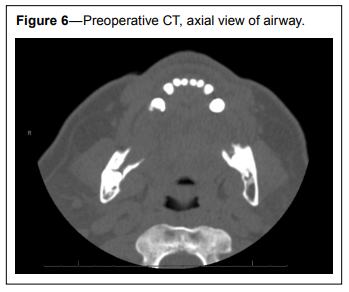
Lateral cephalogram (Figure 5) revealed a hypoplastic maxilla and mandible, and an obtuse mandibular plane angle (76.3 degrees, normal 65). Relative airway restriction in the anterior and posterior dimension is also visualized. Computed tomography (CT) scan obtained while the patient was entirely conscious, revealed narrowed upper airway space as well (Figure 6).
Figure 5Preoperative lateral cephalometric radiograph. |
{kind=link}
Figure 6Preoperative CT, axial view of airway. |
{kind=link}
Due to the occlusal findings, the traditional orthognathic acrylic splint fabrication was difficult. Using the 14 teeth that were erupted with only 4 actually in occlusion, both the interim and final acrylic splints were made using these contacts as well as full contact with the attached gingival overly both the upper and lower alveolus. With so few erupted teeth, both preoperative orthodontics and intraoperative archbars were not possible for stabilization of the splints and the arches in their new position. Thus, intermaxillary fixation screws were planned for intraoperative stabilization.
Surgical treatment was performed under general anesthesia using a nasal endotracheal tube. Intermaxillary screws were placed first; 4 in the maxilla and 4 in the mandible, all 8 mm in length. The traditional horizontal incision and osteotomy were performed at the LeFort 1 level. As per usual surgical protocol, a double guarded nasal osteotome was used to separate the nasal septum from the nasal crest of the maxilla. The single guarded osteotome was then used to separate the lateral nasal wall/medial maxillary sinus wall. A small, then large, curved osteotome was used to separate the maxilla from the pterygoid plates, and a Rowe disimpaction forceps was used to disimpact that maxilla. Given the location of the multiple supernumerary teeth, many were included in the osteotomy and left in place. The interim acrylic splint was placed into the mouth and wired in placed using the intermaxillary fixation wires. After adjusting and enlarging the piriform aperture, the maxilla was held up and into the final planned position, 10 millimeters anterior to the preoperative position, and secured with 4 L-shaped mini plates and 16 six-millimeter screws. The interim splint was removed and the maxilla was found to be stable in the new position.
The surgery was continued with bilateral sagittal split osteotomy of the mandible. Once again, the tradition approach and osteotomies were used. A proper split was obtained bilaterally and both the inferior alveolar nerve and full bony impacted teeth #17 and 32 were visualized and free of trauma. Given the highly impacted nature of these impacted teeth and the expected subsequent weakening of the mandible, they were left in place. After the final acrylic splint was placed and intermaxillary fixation was complete, the mandible was advanced 10 millimeters and fixated in place using 3 bicortical screws on the superior aspect of the mandible placed transcutaneously using a trocar. The intermaxillary fixation wires and intermaxillary fixation screws were removed in totality. The patient was advised to follow a liquid diet protocol during the 5 weeks postoperatively then was to resume normal diet.
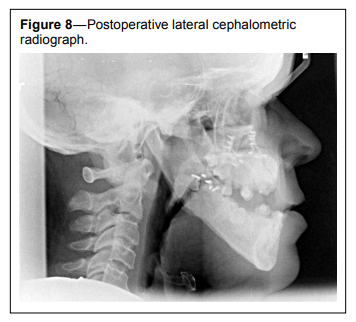
The patient reported feeling more rested with less daytime somnolence within the first week postoperatively. He continued to improve over the first several weeks and transitioned easily from full liquid diet to solids as instructed. He reported easily working 12-hour shifts without the fatigue he used to feel prior to surgery. His mood was elevated and his outlook on like more positive. Clinically he appeared to be well-healed from a surgical standpoint, with no mobility of the segments, no mucosal dehiscence, no signs or symptoms of active infection. His postoperative radiographs revealed stable hardware and no acute or chronic complications of the teeth in the line of osteotomy (Figures 7–12).
Figure 7Postoperative orthopantogram radiograph. |
{kind=link}
Figure 8Postoperative lateral cephalometric radiograph. |
{kind=link}
Figure 9Postoperative posterior-anterior skull radiograph. |
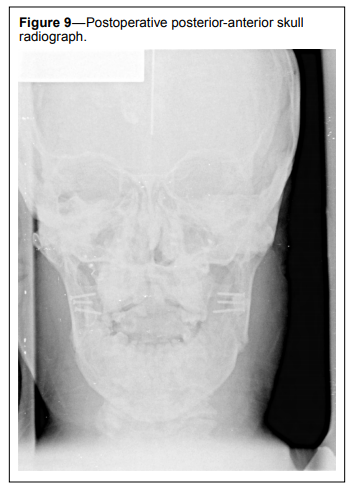{kind=link}
Figure 10Postoperative facial photograph, frontal view. |
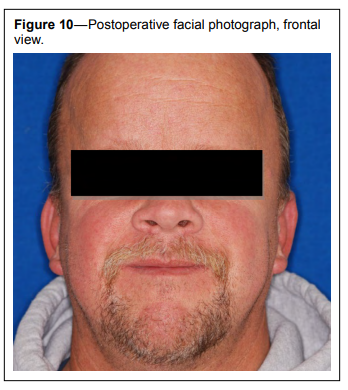{kind=link}
Figure 11Postoperative facial photograph, lateral view. |
{kind=link}
Figure 12Postoperative intraoral photograph, frontal view in occlusion. |
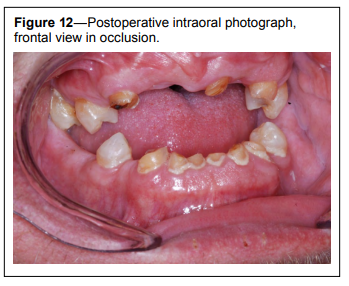{kind=link}
On follow-up polysomnogram, done December 2013, the AHI dropped down to 21 episodes per hour of sleep, with only 3 minutes 45 seconds with an oxygen saturation below 90%, and a total sleep time (TST) of 394 minutes (Table 1).
Table 1Comparison of preoperative and postoperative sleep study measures. |
{kind=link}
DISCUSSION
It is well documented in the literature that maxillomandibular advancement (MMA) surgery increases anterior-posterior and medial-lateral airway size, which can help improve or eliminate OSA.7,8 In 2013, Sittitavornwong et al. demonstrated that, independent of age or gender, all patients who underwent MMA, showed an increase in airway cross-sectional area and a decrease in the pressure effort at every airway level after MMA. In general, as the airway obstruction worsens, a greater pressure effort is required to inspire a normal volume of air. Increasing the 3-dimensional airway space, should decrease this pressure effort, thus decreasing the work of breathing.9 By changing the skeletal framework, MMA increases the pharyngeal space, pulling the tongue and suprahyoid muscles anteriorly. It is currently felt to be the most effective surgical technique for the treatment of obstructive sleep apnea.10,11
There is a significant evidence that early treatment of the dental signs of cleidocranial dysostosis, including multiple supernumerary teeth, malformed dentition, and failure of eruption of teeth, is beneficial to both the aesthetics and longterm functionality of patients.12,13 Extraction of supernumerary teeth, exposure of impacted teeth with traction and orthodontics can lead to a stable long-term occlusion when patients are treated in the prepubescent and early teen years.14
A direct cause and effect link between cleidocranial dysostosis and obstructive sleep apnea has never been established. It does not seem that OSAS is one of the clinical manifestations of the syndrome. Age, gender, and certainly obesity are all well documented to be correlated with OSA.15–17 The prevalence of moderate or severe OSA in the elderly has been reported in the 7% to 44% range, with a much lower influence from BMI/ obesity.18 In the Caucasian population, the cutoff value of BMI for obesity is 30 kg/m2 , and has been reported as low as 23 kg/ m2 in some Asian-Indian populations.19 With the aging population and increasing obesity prevalence, we will certainly see an overall increase in OSAS, including patients born with cleidocranial dysostosis. In patients with cleidocranial dysostosis that have been treated with early intervention for the supernumerary, malformed, and impacted teeth, the traditional maxillomandibular advancement surgery approach would be simple to apply. In those patients that have no previously been treated and present with many unerupted teeth and without a stable occlusion, the surgical planning can be complicated. As seen in this case report, maxillomandibular advancement surgery via the conventional approach, leaving the unerupted teeth within the osteotomy sites both during downfracture/sagittal split and during fixation, can be effective in treating and improving severe OSA.
CONCLUSION
In the setting of severe obstructive sleep apnea, cleidocranial dysotosis is not a contraindication for maxillomandibular advancement surgery, even with the presence of multiple impacted and missing teeth.REFERENCES
2. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population healthy perspective. Am J Respir Crit Care Med 2002;1:165,1217–39.
3. Doff M, Jansma J, Schepers R, Hoekema A. Maxillomandibular advancement surgery as alternative to continuous positive airway pressure in morbidly severe obstructive sleep apnea: a case report. J Craniomandib Sleep Pract 2013;31:246–51.
4. Sleep-related breathing disorders in adults: recommendations for syndrome definition and measurement techniques in clinical research. The Report of an American Academy of Sleep Medicine Task Force. Sleep 1999;22:667–89.
5. National Library of Medicine (US). Genetics Home Reference. Cleidocranial Dysplasia. Reviewed January 2008. Accessed Nov. 14, 2014. Available from: http://ghr.nlm.nih.gov/condition/ cleidocranial-dysplasia.
6. Pagon RA, Adam MP, Ardinger HH, et al. GeneReviews, Cleidocranial Dysplasia. Seattle, WA: University of Washington, 1993–2015.
7. Schendel S, Broujerdi J, Jacobson R. Three-dimensional upper-airway changes with maxillomandibular advancement for obstructive sleep apnea treatment. Am J Orthod Dentofacial Orthop 2014;146:385–93.
8. Bianchi A, Betti E, Tarsitano A, Morselli-Labate AM, Lancellotti L, Marchetti C. Volumetric three-dimensional computer tomographic evaluation of the upper airway in patients with obstructive sleep apnea syndrome treated by maxillomandibular advancement. Br J Oral Maxillofac Sug 2014;52:831–7.
9. Sittitavornwong S, Waite P, Shih A, et al. Computational fluid dynamic analysis of the posterior airway space after maxillomandibular advancement for obstructive sleep apnea syndrome. J Oral Maxillofac Surg 2013;7:1397–405.
10. Li K. Surgical management of obstructive sleep apnea. Clin Chest Med 2003;24:365–70.
11. Butterfield KJ, Marks PL, McLean L, Newton J. Pharyngeal airway morphology in healthy individuals and in obstructive sleep apnea patients treated with maxillomandibular advancement: a comparative study. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;119:285–92.
12. Balaton G, Tarjan I, Balaton P, Barabasi Z, Gyulai G, Nagy K, Vajo Z. Orthodontic and oral surgery therapy in cleidocranial dysplasia. Fogory Sz 2007;100:17–21.
13. Mortellaro C, Greco L, Prota E. Differing therapeutic approaches to cleidocranial dysplasia (CCD). Minerva Stomatol 2012;61:155–63.
14. Zhang CY, Si Y, Wang XZ, Sun XY, Yan WJ, Zheng SG. Early dental treatments for patients with cleidocranial dysplasia. Chin J Dent Res 2014;18:51–7.
15. Bixler EO, Vgontzas AN, Ten Have T, Tyson K, Kales A. Effects of age on sleep apnea in men. Am J Respir Crit Care Med 1998;157:144–8.
16. Dancey DR, Hanly PJ, Soong C, Lee B, Shepard J Jr, Hoffstein V. Gender differences in sleep apnea: the role of neck circumference. Chest 2003;123:1544–50.
17. Romero-Corral A, Caples SM, lopez-Jimenez F, Somer VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest 2010;137:711–9.
18. Duran J, Esnaola S, Rubio R, Iztueta A. Obstructive sleep apneahypopnea and related clinical features in a population-based sample of subjects aged 30 to 70 yr. Am J Respir Crit Care Med 2001;163:685–9.
19. Snehalatha C, Viswanathan V, Ramachandran A. Cutoff values for normal anthropometric variables in Asian Indian adults. Diabetes Care 2003;26:1380–4.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication November, 2015
Accepted for publication February, 2016
Address correspondence to: Heather Chance, DMD, 5318 NC Hwy 55, Suite 106, Durham, NC 27713; Tel: (919) 806-2912; Fax: (919) 806-2915
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest. Case Report performed at the University of Rochester, Strong Memorial Hospital.
PDF