Case Report 1, Issue 3.1
Remote Controlled Mandibular Positional Device to Determine Oral Appliance Efficacy and Therapeutic Protrusive Position
http://dx.doi.org/10.15331/jdsm.5370
James J. Hogg, DDS
Midwest Dental Sleep Center, Chicago, IL
ABSTRACT
Oral appliance therapy (OAT) for obstructive sleep apnea (OSA) has risen with the recent publication research confirming the positive effect of OAT on blood pressure and cardiovascular mortality. The problems that dentists and physicians face are in determining who will be responsive and what target protrusive position is most efficacious for the patient. This is a case report using a remote controlled mandibular positioning device to determine efficacy and the therapeutic or target protrusive position for the patient’s oral appliance.
Keywords:
remote controlled mandibular repositioner
Citation:
Hogg JJ. Remote controlled mandibular positional device to determine oral appliance efficacy and therapeutic protrusive position. Journal of Dental Sleep Medicine 2016;3(1):29–30.
INTRODUCTION
In order to determine the final treated position, most of the early research studies on oral appliance therapy (OAT) for obstructive sleep apnea (OSA) relied on self-titration to a setting where patients reported a relief of symptoms. Patients often make comments at follow-up visits such as “My wife says I am not snoring, and I feel great, so I am sure my appliance is working.” According to early studies, this kind of patient feedback would have directly corresponded to the determination of the patient’s final treated position. However, Almeida reported that 17% to 35% of these patients require further calibration beyond the point where subjective symptoms are resolved in order to reach objective efficacy.1
The dentist is always faced with the dilemma of where to start the protrusive position of the oral appliance and how far to calibrate the device to reach an objective efficacious position. Fleury2 used subjective observations and oximetry to determine this position, which often yielded positive results. Unfortunately, despite those positive results, Fleury’s method does not always result in an OAT titration polysomnogram (PSG) that demonstrates resolution of OSA. This may be due to night-to-night variability and/or the inability of oximetry to accurately record total sleep time, sleep stages, or positional data.
Calibration of the appliance during a single night manual titration PSG, as used by Almeida, has proven to significantly improve OAT outcomes. Despite the improvement, there are limitations to these studies. In clinical practice, single-night manual titration PSG is inconsistent and impractical. It is inconsistent due to the lack of a single standardized protocol for the calibration of an oral appliance. In an urban setting, there are a multitude of sleep laboratories with varying degrees of experience calibrating appliances. The lack of standardization creates inconsistent terminology, protocols that change with the type of appliance, and the preference of each dentist referring into the lab. It is impractical because it disregards the significance of frequent disruptions to the patient’s sleep architecture during each calibration. This lack of standardization and disruption of the patient’s sleep creates uncertainty in the reliability and practicality of the study itself.
REPORT OF CASE
This case used a remote controlled mandibular positioning device (MATRx)3 during PSG, which differed from previous calibration methods in that the patient was calibrated prior to the fabrication of a custom oral appliance. This enabled the sleep physician to determine whether the patient was responsive to oral appliance therapy and to then identify the target protrusive position that was most efficacious. The patient was a 30-year-old man who had a BMI of 37.9. His medical history was unremarkable except for a diagnosis of GERD. He had been diagnosed with moderate OSA: AHI (apnea hypopnea index) = 22.1, REM AHI = 32.2, O2 nadir = 82%. He had trialed CPAP at a pressure of 14 cm but was noncompliant due to mask leakage and noise disruptions to his pregnant wife. Previous studies by Sutherland4 and Tsuiki5 would identify this patient as a potential failure with OAT due to the high CPAP pressure. However, due to his noncompliance with CPAP, the patient was referred to me by his sleep physician for a dental evaluation and fitting of the MATRx calibration trays for the study.
The patient had good periodontal health, a Class III occlusion on the right side, Class I on the left, and a bilateral cross bite. His tongue was Level III, tonsils Level III, and Mallampati Level II with an edematous and wide uvula. His soft palate was elongated with a lack of tone, his hard palate was vaulted, and his oropharynx was crowded. After the evaluation, stock MATRx trays were fabricated using bite registration material for the impressions. His maximum protrusive range was 9 mm. Using the MATRx mm ruler (10–20 mm), his range was determined to be 10 mm. The sleep lab technician was instructed to begin calibration at 60% of his maximum protrusive range.
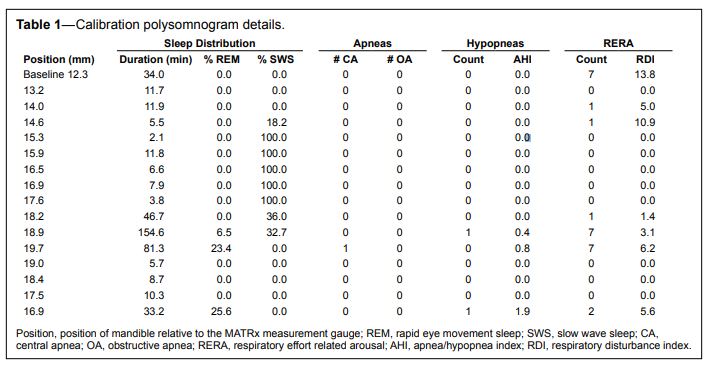
During the PSG, the appliance was advanced in 0.6 mm (0.2 mm × 3) increments.3 The goal was to stabilize the respiratory events to ≤ 1 apnea or hypopnea during a 5-minute window of supine REM sleep. The patient’s final position was 19.7 mm (MATRx scale) or 1 mm from his maximum protrusive range (8 mm of protrusion).
The PSG results showed resolution of OSA: AHI = 0, REM AHI = 0, RDI = 6.2, O2 nadir = 91 (Table 1).
Table 1Calibration polysomnogram details. |
{kind=link}
The patient had a TAP 3 TL oral appliance delivered at 5 mm from his maximum protrusive position. Following a one week acclimation period, the patient was instructed to begin advancing the appliance 1–2 turns (0.25–0.5 mm) every other night for a total of 20 turns. This would advance the appliance to his therapeutic treatment position of 1 mm from maximum protrusion. At the one month follow-up, he reported feeling rested (Epworth = 0) and noted that his wife was happy as his snoring was gone.
Three months after delivery, the patient had an ARES home sleep test for one night at the treated position. His results were as follows: AHI = 2, RDI = 12, O2 nadir = 89. Due to his increased RDI and slight return of light snoring, the sleep physician suggested further titration. After 2 additional turns (0.5 mm), the patient’s snoring was controlled.
He was seen 6 months later and was well rested with an Epworth of 0, and his BMI had dropped to 34.70. He was now 2.5 mm from his maximum protrusive as he had had 2 mm of horizontal change forward in his overjet. He was therefore encouraged to use his morning bite repositioner on a more regular basis.
CONCLUSION
The use of a remote controlled mandibular positioner (MATRx) provided a standardized, reliable, and practical solution for predicting the efficacy and target protrusion in single night PSG. It also allowed for remote calibration through the specified range of motion without significantly disturbing the patient’s sleep architecture. The patient’s high BMI, crowded oropharynx, large tongue, and severe AHI in REM may have dissuaded many physicians from prescribing OAT. However, the MATRx provided objective efficacy data at specific protrusive positions allowing the sleep physician to confidently prescribe OAT at a predetermined target protrusion. In addition, it provided the objective data needed to fabricate the custom appliance to the ordered target protrusion.
REFERENCES
2. Fleury B, Rakotonanahary D, Petelle B, et al. Mandibular advancement titration for obstructive sleep apnea: optimization of the procedure by combining clinical and oximetric parameters. Chest 2004;125:1761–7.
3. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep 2013;36:1517–25.
4. Sutherland K, Phillips CL, Davies A, et al. CPAP pressure for prediction of oral appliance treatment response in obstructive sleep apnea. J Clin Sleep Med 2014;10:943–9.
5. Tsuiki S, Kobayashi M, Namba K, et al. Optimal positive airway pressure predicts oral appliance response to sleep apnoea. Eur Respir J 2010;35:1098–105.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication August, 2015
Submitted in final revised form September, 2015
Accepted for publication September, 2015
Address correspondence to: James J. Hogg, DDS, Diplomate, ABDSM, Dental Director, Midwest Dental Sleep Center, Chicago, IL 60611; Email: drjamesjhogg@gmail.com
DISCLOSURE STATEMENT
This was not an industry supported study. Dr. Hogg received an honorarium from Zephyr Sleep Technologies to present at their Chicago symposium and at the Southern Sleep Society meeting in New Orleans. Dr. Hogg has indicated no financial conflicts of interest.
PDF