Case Report 1, Issue 13.1
Multidisciplinary Treatment of Obstructive Sleep Apnea and Restoring Oral Volume
http://dx.doi.org/10.15331/jdsm.7424Shahrzad Salartash, DDS, MAGD, NMD, D. ABDSM1
1Dynamic Dental Wellness, 20755 Williams Port place #300, Ashburn, VA
ABSTRACT
Obstructive sleep apnea (OSA) is a complex condition often associated with comorbid dental issues such as malocclusion and bruxism. Effective management requires a comprehensive, individualized approach that considers anatomical, medical, behavioral, and lifestyle factors. This case report details the successful treatment of a patient with OSA who is intolerant to continuous positive airway pressure through a multidisciplinary protocol combining oral appliance therapy, maxillary expansion, restoration of vertical dimension of occlusion, nonablative soft-tissue laser therapy, orofacial myofunctional therapy, and collaboration with a postural restorative physical therapist. The integrated approach resulted in marked improvements in both sleep quality and airway function. This case underscores the importance of incorporating dental, functional, and postural considerations into the management of OSA, and supports the value of interdisciplinary collaboration in achieving optimal patient outcomes.
Keywords:
obstructive sleep apnea treatment, misaligned teeth, adult orthopedic maxillary expansion treatment, soft tissue none ablative laser therapy, restoring oral volume, multidisciplinary approach, myofunctional therapy, and physical therapy.
Citation:
Salartash S, Multidisciplinary Treatment of Obstructive Sleep Apnea and Restoring Oral Volume. J Dent Sleep Med. 2026;13(1)
INTRODUCTION
Sleep plays a fundamental role in human health, development, and overall well-being. Sleep-disordered breathing (SDB) is the most prevalent category of sleep disorders and has been increasingly associated with a wide range of systemic health concerns. Among these, obstructive sleep apnea (OSA) is particularly concerning because of its impact on physical health, cognitive function, and neuropsychomotor development, especially in children. Left untreated, OSA can lead to significant long-term consequences, including cardiovascular, metabolic, and behavioral disorders.1-6
Traditional treatments such as adenotonsillectomy and continuous positive airway pressure (CPAP) have demonstrated benefits but often fail to fully resolve the underlying anatomical and functional contributors to the disorder.5-6 As understanding of OSA pathophysiology evolves, there has been growing interest in minimally invasive therapies including oral appliances, myofunctional therapy, and orthopedic orthodontic interventions. Recent studies suggest that techniques such as rapid maxillary expansion and mandibular advancement can effectively increase airway dimensions and reduce the apnea-hypopnea index (AHI), particularly in patients with craniofacial deficiencies. 20-24,37-38,40-41
Emerging evidence supports the integration of dental and myofunctional therapies in the management of OSA, highlighting the importance of a multidisciplinary approach. This case report contributes to the growing body of literature by demonstrating the effectiveness of a personalized, multimodal treatment strategy for OSA that incorporates oral appliance therapy, maxillary expansion, soft-tissue laser therapy, orofacial myofunctional exercises, and postural rehabilitation. The findings emphasize the need for continued research and collaboration across disciplines to optimize outcomes in patients with sleep-disordered breathing.7-10, 20-24, 29-32, 37-48
CASE REPORT
A 67-year-old woman with a diagnosis of severe OSA and intolerance to CPAP therapy was referred for comprehensive evaluation and multidisciplinary treatment. The patient presented with a constellation of symptoms, including chronic coughing, restless leg syndrome, diastolic dysfunction, episodic anoxia, persistent thirst, exertional dyspnea, recurrent sinus infections, and frequent eye irritation, which she attributed to air leakage from her CPAP mask. Her primary concern was nocturnal oxygen desaturation, further exacerbated by a family history of dementia. Her initial body mass index (BMI) was recorded at 27 kg/m2.
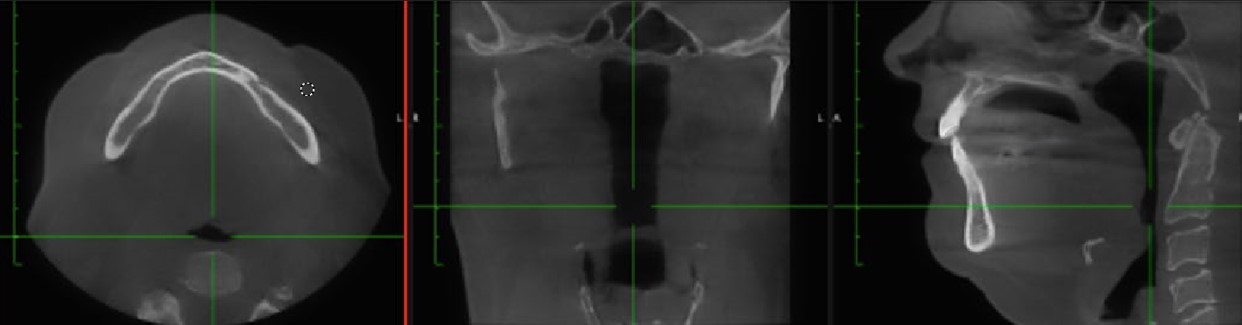
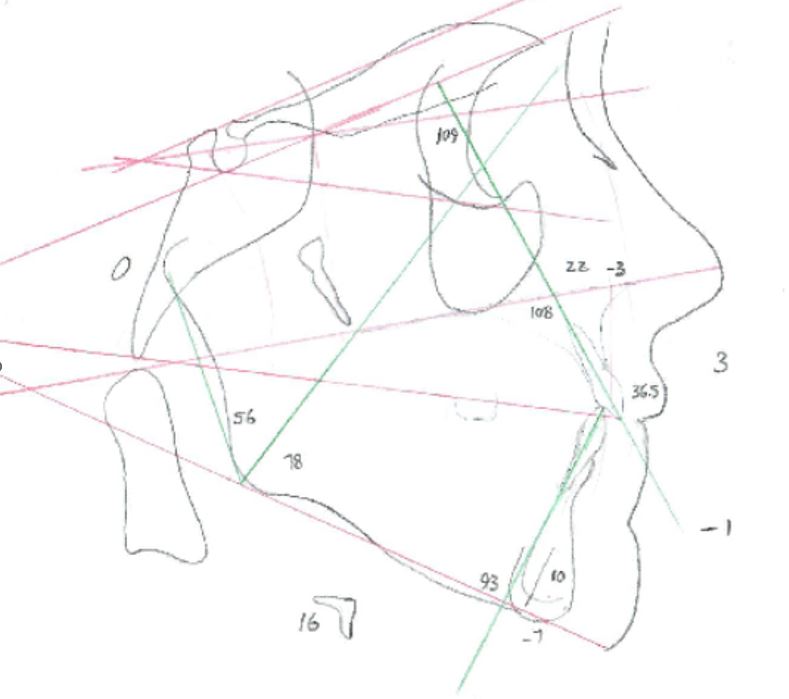
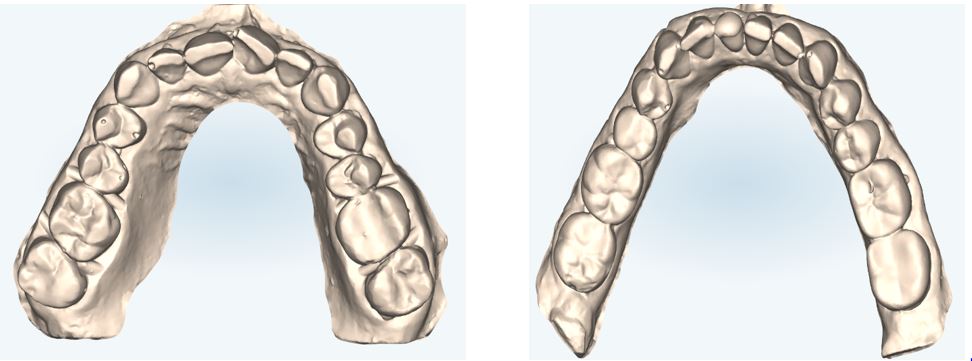
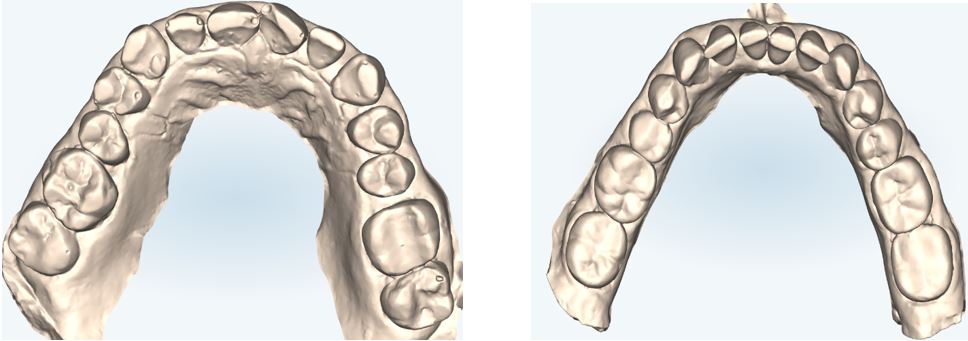
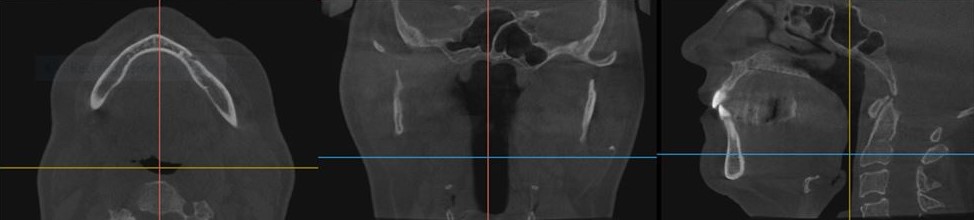
Initial cone beam computed tomography (CBCT) revealed low tongue posture (Figure 1). Figures 2, 3, and 4 show the frontal, maxillary occlusal, and mandibular occlusal views of the dentition, respectively. Clinical examination identified a scalloped tongue with low muscle tone and difficulty achieving palatal suction. Dental findings included upper and lower arch crowding, advanced tooth wear consistent with attrition, a deep skeletal bite evident on cephalometric analysis, and a marked loss of vertical dimension of occlusion (VDO) (Figures 5 and 6).
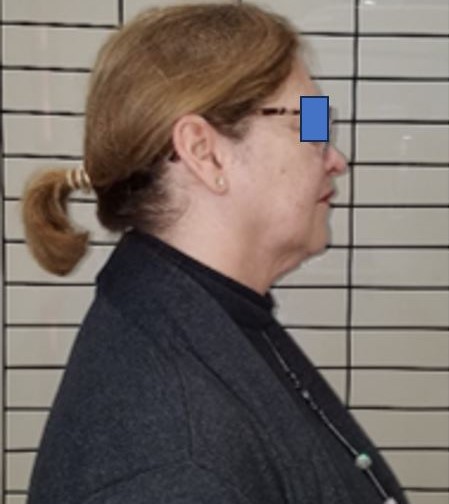
The patient exhibited forward head posture (FHP) measured at 7 cm anterior to the cervical spine by assessing the position of the external auditory meatus relative to the acromion process. This anterior shift in craniovertebral alignment contributes to compromised oral posture and impaired airway function. FHP is closely associated with mandibular misalignment, cervical spine dysfunction, cranial rotation, and upper airway narrowing. Postural instability originating from the stomatognathic system has significant repercussions on airway patency, musculoskeletal equilibrium, and central nervous system regulation.29-36
Studies have reported up to 30% reduction in oxygen intake in individuals with forward head posture. Mechanistically, anterior head shift increases reliance on accessory respiratory muscles, such as the scalenes, resulting in shallow, thoracic-dominant breathing that limits diaphragmatic engagement and reduces systemic oxygenation. Additionally, FHP often co-occurs with rounded shoulders, which contribute to collapse of the chest wall and compression of the thoracic cavity. This cascade impairs ribcage expansion, restricts diaphragmatic excursion, and diminishes lung capacity.33-35
The clinical significance of head and neck posture on systemic health is increasingly recognized, with documented effects on spinal pain, headache incidence, cardiovascular function (blood pressure and heart rate), mood, and pulmonary efficiency. 33-36 As detailed in the text The Physiology of the Joints, 33 the human head weighs approximately 4.5–5 kg (10–11 lb), but because of the lever arm effect created by anterior displacement of the head’s center of gravity, the resulting compressive load at the cervical spine can reach approximately 42 lb. A forward shift of even 5 to 7.5 cm (2 to 3 inches) from neutral posture significantly increases mechanical strain on cervical structures, amplifying postural and functional impairments.33
Home sleep apnea testing reported an AHI of 41.7 events/hour, with a supine AHI of 51.9 events/hour, an oxygen saturation nadir of 81%, and a respiratory disturbance index of 42.1. Radiologic interpretation of the CBCT confirmed a deviated nasal septum, severe oropharyngeal narrowing at the level of the soft palate and posterior third of the tongue, and lingual tonsillar hypertrophy. Cervical spine imaging also demonstrated intervertebral foraminal stenosis at levels C3–C5 and joint space narrowing—findings consistent with chronic forward head posture and its biomechanical consequences.32-35
Figure 1. |
{kind=link}
Figure 2. |
{kind=link}
Figure 3. |
{kind=link}
Figure 4. |
{kind=link}
Figure 5. |
{kind=link}
Figure 6. |
{kind=link}
Figure 7. |
{kind=link}
TREATMENT PLAN
Two primary treatment options were presented to the patient, along with two adjunctive therapies:Option 1: Oral Appliance Therapy
A dorsal oral appliance was proposed to advance the mandible and tongue during sleep, thereby reducing upper airway obstruction. Although this method could mitigate OSA symptoms, it would not correct the underlying skeletal, dental, or postural factors contributing to airway collapse.9
Option 2 (Selected by the Patient): Maxillary Expansion and Mandibular Repositioning With Full-Mouth Rehabilitation
This comprehensive approach aimed to restore craniofacial architecture, optimize airway patency, and reestablish functional occlusion. Treatment included the following phases:
Orthopedic Maxillary Expansion and Mandibular Repositioning
Treatment was initiated using an Advanced Lightwire Functional (ALF) appliance combined with a neuromuscular mandibular orthotic.10-28 This dual-therapy protocol was designed to:
- Address transverse maxillary constriction
- Reestablish VDO
- Achieve true orthopedic (skeletal) expansion while minimizing buccal dental tipping
- Reposition the mandible and tongue to optimize upper airway volume 9-22,45-49 (Figure 5)
- ALF and orthotic adjustments were performed monthly (Figure 7).
- Expansion was achieved incrementally at 0.25-mm intervals, measured at the first molar width (UR1M–UL1M) using dental calipers.
- The patient reported high compliance with only transient hypersalivation and mild discomfort during adaptation.
Neuromuscular Bite Registration and Full-Mouth Rehabilitation
A physiologic bite was established using the Myotronics TENS protocol to determine an optimal neuromuscular mandibular position. Goals included:
- Relaxation of hypertonic masticatory muscles
- Neuromuscular reprogramming of jaw proprioception
- Establishment of a stable mandibular rest and occlusal position
- Electrodes placed on the masseter, temporalis, digastric, and lateral pterygoid muscles
- Parameters: 2 to 10 Hz frequency; 50 to 70 µs pulse width
- Duration: 20 to 30 minutes per session
- Bite registration taken at 1 to 2 mm above physiologic rest (freeway space) using Myo-Print™
- Resting anterior temporalis and masseter electromyography values were within normal physiologic range.
- Full-mouth prosthetic reconstruction followed to restore functional occlusion and VDO.
- Shimbashi measurement (CEJ #9 to CEJ #24) improved from 13.10 mm to 18.38 mm, indicating a 5.28-mm increase in vertical dimension.
ADJUNCTIVE THERAPIES (SELECTED BY THE PATIENT WITH OPTION 2)
Postural Restorative Physical Therapy and Myofunctional Therapy
The patient opted to address functional deficits contributing to compromised airway dynamics and posture. Goals of interdisciplinary therapy included:
- Improving craniocervical alignment and reducing forward head posture
- Strengthening tongue tone and mobility
- Reestablishing nasal breathing and passive lip seal8,44-45
- Encouraging diaphragmatic breathing for autonomic regulation30-36
Referrals were made to a postural physical therapist and certified orofacial myofunctional therapist.
NightLase® Laser Therapy
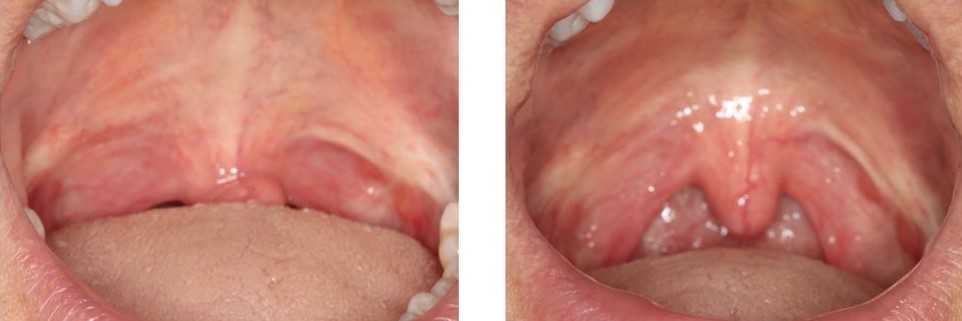
Five sessions of Er:YAG laser treatment were administered to the soft palate and oropharynx at 21-day intervals. The NightLase® protocol was designed to:
- Stimulate collagen remodeling via photothermal effect
- Tighten oropharyngeal soft tissues nonsurgically
- Enhance airway patency and reduce upper airway collapsibility 42-43 (Figure 10)
OUTCOMES AND FOLLOW-UP
Posttreatment CBCT, cephalometric and Schwartz model analysis revealed:
- Maxillary expansion (Figure 8-9)
- Improved mandibular positioning (Figure 12)
- Tongue resting posture against the palate (Figure 12)
Home Sleep Apnea Test Results:
- AHI reduced from 41.7 to 9 events/hour
- Supine AHI: 51.9 to 0 events/hour
- Oxygen desaturation index: 21.3 to 4
- O2 saturation nadir: 81% to 93%
Arch Width and Oral Volume Increase (Schwartz Model Analysis):
- Premolar width (mesial pit #5–#12): 30.86 mm → 36.81 mm (+5.95 mm) (Figure 9)
- First molar width (#3–#14): 40.59 mm → 46.24 mm (+5.65 mm) (Figure 8-9)
- VDO increase: 5.28 mm (Figure 11)
- Oral volume increase: estimated at 25 mm²
Postural Improvements:
Additional Notes:
- Ear, Nose, and Throat referral declined because of prior unsuccessful septoplasty
- No signs of dental tipping postexpansion (Figure 8-9)
- Patient followed biannual recall schedule per AADSM guidelines
- Annual NightLase® maintenance recommended
- Patient BMI stayed the same at 27 kg/m2.
Symptom improvement was reported to be incremental rather than immediate. Initial changes such as reduced snoring and daytime fatigue were noticed within the first few months of orthopedic appliance therapy, but the most significant improvements—including normalized Epworth Sleepiness Scale scores and reduced AHI—were observed after completion of the full treatment protocol. This suggests that airway remodeling and neuromuscular adaptation may require cumulative and progressive changes rather than instantaneous correction.
Figure 8. |
{kind=link}
Figure 9. |
{kind=link}
Figure 10. |
{kind=link}
Figure 11. |
{kind=link}
Figure 12. |
{kind=link}
Figure 13. |
{kind=link}
Figure 14. |
{kind=link}
DISCUSSION
This case highlights the value of a comprehensive, multidisciplinary approach in managing a complex presentation of OSA in conjunction with dental malocclusion and loss of VDO. The integration of an upper ALF appliance and a lower neuromuscular mandibular orthotic enabled simultaneous correction of oral volume deficiency and posterior tongue collapse—two key contributors to airway obstruction in OSA.Clinical Outcomes and Airway Improvement
The patient demonstrated a significant reduction in the AHI, from a severe to a clinically minimal range, with complete resolution of supine AHI. These findings indicate substantial improvement in airway patency and sleep quality. The use of functional and orthopedic dental appliances not only alleviated malocclusion and restored VDO but also facilitated structural changes that contributed to long-term airway stability.
Multidimensional Therapeutic Strategy
Although combining oral appliance therapy with orthodontic and restorative interventions remains debated, this case supports the efficacy of targeted dental expansion and mandibular repositioning in addressing interrelated issues including:
- Dental crowding
- Reduced oral volume
- Compromised tongue posture
- Airway obstruction
Forward Head Posture and Craniofacial Biomechanics
The patient exhibited FHP (Figure 13), with the external auditory meatus positioned approximately 7 cm anterior to the vertical line aligned with the acromion and cervical spine. This measurement was obtained using plumb line and photographic postural analysis, a validated method for evaluating craniovertebral angle and sagittal head deviation.33
FHP exerts a well-documented influence on mandibular alignment, oral volume, and upper airway stability. It contributes to:
- Altered respiratory mechanics
- Reduced diaphragmatic excursion
- Oxygen desaturation
- Increased cervical muscle strain
- Spinal misalignment
- Autonomic dysregulation
Nasal Breathing, Lip Competency, and Tongue Posture
Nasal breathing, lip competency, and optimal tongue posture are foundational to orofacial and airway health. Their therapeutic optimization was central to this case:
- Nasal breathing promotes nitric oxide production, supports craniofacial development, and reduces inspiratory resistance by improving filtration and humidification of air. 44 Chronic mouth breathing is associated with maxillary constriction, altered tongue posture, and increased risk of sleep-disordered breathing.46
- Lip competency, or maintaining a gentle lip seal at rest, is vital for intraoral pressure regulation and orofacial muscle tone. Incompetent lips can lead to vertical growth tendencies and perpetuate malocclusion and airway compromise.47
- Tongue posture and function influence oral volume, palatal development, and oropharyngeal space. A properly postured tongue resting on the palate exerts lateral pressure to support maxillary width and a patent airway. In contrast, low or retracted tongue posture is associated with high-arched palates and airway narrowing. Tongue tone and mobility are also critical for proper swallowing, speech, and airway protection. 45,48
Expansion versus tipping: Although ALF appliances are sometimes associated with buccal tipping rather than true skeletal expansion, this case demonstrated quantifiable increases in intermolar and interpremolar width without clinical signs of buccal crown flaring or root exposure. Expansion measurements were performed using calipers and confirmed via CBCT and Schwartz model analysis. However, given the design limitations of the ALF appliance, some degree of dental tipping cannot be entirely ruled out and should be acknowledged as a potential limitation of the orthopedic phase of treatment. Careful activation by a practitioner trained in ALF protocol is critical to achieving skeletal outcomes.
Therapies such as myofunctional training, oral appliances, and breathing retraining are thus instrumental in restoring these foundational functions and improving long-term airway dynamics.
Clinical Implications and Future Directions
This case has implications for both general and dental sleep medicine practitioners, especially in managing patients who are CPAP-intolerant or undergoing presurgical evaluation for OSA. The treatment model presented here offers a viable, noninvasive alternative or adjunct to traditional therapies, yielding functional, aesthetic, and physiological benefits.
Further research with larger sample sizes and extended follow-up is warranted to validate these findings and to develop standardized protocols for incorporating airway-focused dental therapy into broader OSA management strategies.
CONCLUSION
Management of OSA must include an assessment of contributing dental factors such as malocclusion and structural tooth loss due to attrition. As this case illustrates, individualized treatment planning that considers the patient's anatomy, functional needs, and overall health can lead to significant therapeutic gains. The integration of oral appliance therapy, NightLase® soft-tissue laser treatment, orofacial myofunctional therapy, physical therapy, and vertical dimension restoration proved effective in addressing both the airway obstruction and underlying dental conditions. This multidisciplinary approach supports the growing role of dental professionals in the collaborative care of patients with sleep-disordered breathing. It further emphasizes the importance of a comprehensive, patient-centered model in the advancement of dental sleep medicine.
This case was a success but more research with larger sample sizes and long-term follow-up are warranted to validate these outcomes and develop standardized protocols for integrating airway-focused dental therapy into OSA management strategies.
REFERENCES
- Balasubramaniam R, Klasser GD, Cistulli PA, Lavigne GJ. The link between sleep bruxism, sleep disordered breathing and temporomandibular disorders: An evidence-based review. J Dent Sleep Med. 2014;1(1):27–37.
- Cohen-Levy J, Quintal MC, Rompré P, Almeida F, Huynh N. Prevalence of malocclusions and oral dysfunctions in children with persistent sleep-disordered breathing after adenotonsillectomy in the long term. J Clin Sleep Med. 2020;16(8):1357-1368. doi:10.5664/jcsm.8534
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328(17):1230-1235. doi:10.1056/NEJM199304293281704
- Weaver TE, Grunstein RR. Adherence to continuous positive airway pressure therapy: The challenge to effective treatment. Proc Am Thorac Soc. 2008;5(2):173-178. doi:10.1513/pats.200708-119MG
- Leck R, Paul N, Rolland S, Birnie D. The consequences of living with a severe malocclusion: A review of the literature. J Orthod. 2022;49(2):228-239. doi:10.1177/14653125211042891
- Kandasamy S, Goonewardene M. Class II malocclusion and sleep disordered breathing. Semin Orthod. 2014;20(4):316-323. doi:10.1053/j.sodo.2014.09.007
- Ataii P. Performing orthodontics while treating OSA. Inside Dentistry. 2019;15(2).
- Lee Y-C, Lu C-T, Cheng W-N, Li H-Y. The impact of mouth-taping in mouth-breathers with mild obstructive sleep apnea: A preliminary study. Healthcare (Basel). 2022;10(9):1755. doi:10.3390/healthcare10091755
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11(7):773-827. doi:10.5664/jcsm.4858
- Machado Júnior AJ, Crespo AN. Expansion of the maxilla in adults with OSAS: myth or reality? Sleep Med. 2020;65:170-171. doi:10.1016/j.sleep.2019.06.014
- Lin L, Ahn HW, Kim SJ, Moon SC, Kim SH, Nelson G. Tooth-borne vs bone-borne rapid maxillary expanders in late adolescence. Angle Orthod. 2015;85(2):253-262. doi:10.2319/030514-156.1
- Türker G, Çoban G, Bayraktar AÜ, et al. Three-dimensional palatal morphology and upper arch changes following nonsurgical and surgical maxillary expansion in adults. Oral Surg Oral Med Oral Pathol Oral Radiol. 2022;134(4):425-431. doi:10.1016/j.oooo.2022.02.013
- Delz E. The ALF (Advanced Lightwire Functional Appliance) creating facial beauty and balance. Int J Orthod Milwaukee. 2009;20(2):23-27.
- Nordstrom D. Positive alveolar and gingival effects of the ALF-LB. Funct Orthod. 1996;13(5):4-6, 8.
- Smith GH, Ashton H. Alternative lightwire functionals (ALF). Funct Orthod. 1995;12(4):35-38.
- Goodman P. The ALF appliance. Funct Orthod. 1995;12(2):30-36.
- James GA, Strokon D. The significance of cranial factors in diagnosis and treatment with the advanced lightwire functional appliance. Int J Orthod Milwaukee. 2003;14(3):17-23.
- Turzo T. The ALF approach. Cranio. 2019 Mar;37(2):72-73. doi: 10.1080/08869634.2019.1570638. PMID: 30793674.
- Jolivet C, Nguyen Kim K. L'orthodontie de l'adulte: le traitement global des cas complexes. Traitement prothétique et dysmorphose dento-squelettique [Orthodontics in adults: comprehensive treatment of complex cases. Prosthetic treatment and dento-skeletal dysmorphosis]. Orthod Fr. 1997;68(1):183-96. French. PMID: 9432601
- Dao N, Cozean C, Chernyshev O, Kushida C, Greenburg J, Alexander JS. Retrospective analysis of real-world data for the treatment of obstructive sleep apnea with slow maxillary expansion using a unique expansion dental appliance. Pathophysiology. 2023;30(2):199-208. doi:10.3390/pathophysiology30020017
- Kushida C, Cozean C, Alexander J. 0549 Non-permanent oral appliance treatment of severe obstructive sleep apnea. Sleep. 2024;47(Suppl 1):A235. doi:10.1093/sleep/zsae067.0549
- Heckman S, Katz D, Kushida C. 0340 Non-surgical maxillary expansion using a novel oral appliance system. Sleep. 2022;45(Suppl 1):A153. doi:10.1093/sleep/zsac079.337
- Lee-Heidenreich D, Heckman S, Kushida C. 0530 Efficacy of obstructive sleep apnea treatment by a unique oral appliance and effect of concurrent myofunctional and CPAP therapy. Sleep. 2023;46(Suppl 1):A233-A234. doi:10.1093/sleep/zsad077.0530
- Barone DA. Alternative devices for obstructive sleep apnea. Clin Neurol J. 2013;3(1):67-70. doi:10.1212/CPJ.0b013e318278be88
- Li K, Guilleminault C. Surgical and non-surgical maxillary expansion: expansion patterns, complications and failures. Orthod Fr. 2022;93(Suppl 1):35-46. doi:10.1684/orthodfr.2022.87
- Smith GH, Ashton H. Advanced lightwire functionals reduce orthodontic relapse factor. Funct Orthod. 1996;13(5):16-18, 20.
- Strokon D. ALF correction of facial and postural asymmetry. Int J Orthod Milwaukee. 2010;21(1):39-44.
- James G, Strokon D. Cranial strains and malocclusion VIII: palatal expansion. Int J Orthod Milwaukee. 2009;20:15-30.
- Sökücü O, Okşayan R, Uyar M, et al. Relationship between head posture and the severity of obstructive sleep apnea. Am J Orthod Dentofacial Orthop. 2016;150(6):945-949. doi:10.1016/j.ajodo.2016.05.011
- Saldiran TÇ, Kara İ, Yikilmaz SK, Durgun M. Influence of body posture and apnea severity on the tone and elasticity of upper airway muscles in awake patients with obstructive sleep apnea: A cross-sectional study. J Manipulative Physiol Ther. 2022;45(5):365-377. doi:10.1016/j.jmpt.2022.08.006
- Makofsky HW. Snoring and obstructive sleep apnea: does head posture play a role? Cranio. 1997;15(1):68-73. doi:10.1080/08869634.1997.11745994
- Pham T, Lin CK, Leek D, et al. Obstructive sleep apnea's association with the cervical spine abnormalities, posture, and pain: a systematic review. Sleep Med. 2020;75:468-476. doi:10.1016/j.sleep.2020.09.008
- Kapandji IA. The Physiology of the Joints. Volume 3: The Vertebral Column, Pelvic Girdle and Head. 6th ed. Paris: Elsevier; 2008.
- Kim, S. Y., Koo, S. J., & Jung, J. H. (2018). Effect of forward head posture on forced vital capacity and respiratory muscles activity. Journal of Physical Therapy Science, 30(1), 132–135. https://doi.org/10.1589/jpts.30.132
- Katzman, W. B., Wanek, L., Shepherd, J. A., & Sellmeyer, D. E. (2017). Age-related hyperkyphosis: Its causes, consequences, and management. Journal of Orthopaedic & Sports Physical Therapy, 40(6), 352–360. https://doi.org/10.2519/jospt.2010.3099
- Morad, Y., Avraham, M., & Schliamser, L. M. (2021). The impact of head posture on autonomic nervous system activity: A pilot study. Journal of Back and Musculoskeletal Rehabilitation, 34(3), 415–421. https://doi.org/10.3233/BMR-200345
- Dao N, Cozean C, Chernyshev O, et al. Retrospective analysis of real-world data for the treatment of obstructive sleep apnea with slow maxillary expansion using a unique expansion dental appliance (DNA). Pathophysiology. 2023;30(2):199-208. doi:10.3390/pathophysiology30020017
- Abdullatif J, Certal V, Zaghi S, et al. Maxillary expansion and maxillomandibular expansion for adult OSA: A systematic review and meta-analysis. J Craniomaxillofac Surg. 2016;44(5):574-578. doi:10.1016/j.jcms.2016.02.001
- Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: A systematic review and meta-analysis. Sleep. 2015;38(5):669-675. doi:10.5665/sleep.4652
- Machado-Júnior AJ, Zancanella E, Crespo AN. Rapid maxillary expansion and obstructive sleep apnea: A review and meta-analysis. Med Oral Patol Oral Cir Bucal. 2016;21(4):e465-469. doi:10.4317/medoral.21073
- Cistulli PA, Palmisano RG, Poole MD. Treatment of obstructive sleep apnea syndrome by rapid maxillary expansion. Sleep. 1998;21(8):831-835.
- Jorge JH, et al. NightLase®®: A non-invasive laser treatment for snoring and obstructive sleep apnea. J Lasers Med Sci. 2019;10(2):92–98.
- VukojeviÄ D, et al. The effectiveness of Er:YAG laser in the treatment of snoring: A randomized controlled clinical trial. Clin Oral Investig. 2017;21(6):1729–1736.
- Lundberg, J.O.N., Weitzberg, E. (1999). Nasal nitric oxide in man. Thorax, 54(10), 947–952.
- Guilleminault, C., Huseni, S., & Lo, L. (2016). A frequent phenotype for pediatric sleep apnoea: short lingual frenulum. European Respiratory Journal, 48(6), 188–193.
- Harari, D., Redlich, M., Miri, S., Hamud, T., & Gross, M. (2010). The effect of mouth breathing versus nasal breathing on dentofacial and craniofacial development in orthodontic patients. Laryngoscope, 120(10), 2089–2093.
- Huang, Y.-S., Guilleminault, C. (2013). Pediatric obstructive sleep apnea: Where do we stand? Advances in Oto-Rhino-Laryngology, 80, 144–152.
- Guimarães, K.C., Drager, L.F., Genta, P.R., Marcondes, B.F., & Lorenzi-Filho, G. (2009). Effects of oropharyngeal exercises on patients with moderate obstructive sleep apnea syndrome. American Journal of Respiratory and Critical Care Medicine, 179(10), 962–966.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted March 26, 2025
Submitted in final revised form July 29, 2025
Accepted for publication October 23, 2025
Address correspondence to: Shahrzad Salartash, DDS, MAGD, NMD, D. ABDSM, Dynamic Dental Wellness, 20755 Williams Port place #300, Ashburn, VA. Email: Salartash@gmail.com.