Case Report 1, Issue 1.3
Oral Appliance Therapy and Atrial Fibrillation
http://dx.doi.org/10.15331/jdsm.4136
Kathleen Bennett, DDS, Diplomate, ABDSM
Department of Internal Medicine Division of Pulmonary Sleep Medicine UC Health West Chester Hospital, Cincinnati, OH
ABSTRACT
Atrial fibrillation (AF) is the most common sustained arrhythmia affecting more than two million Americans. Patients have shown significant improvement both pre and post ablation with the use of both medication and CPAP. Non-compliant or non-tolerant CPAP patients may benefit from oral appliance therapy. Case is presented of a patient with AF, who was treated with an oral appliance.
Keywords:
oral appliance
Citation:
Bennett K. Oral appliance therapy and atrial fibrillation. Journal of Dental Sleep Medicine 2014;1(3):121–122.
Atrial fibrillation (AF) is the most common sustained arrhythmia, affecting more than two million Americans. The prevalence of obstructive sleep apnea (OSA) in patients with atrial fibrillation is 32% to 49%. AF prevalence is directly correlated with the severity of obstructive sleep apnea (OSA).1,2 Mechanisms thought to be at least partly responsible for the interaction of AF and OSA include elevated intrathoracic pressure, increased autonomic nervous system activity, and inflammation.3 A trend towards increased AF recurrence has been described in patients with untreated OSA after treatment for AF.4 The risk of AF recurrence is related to the duration of oxygen saturation < 90% and the magnitude of the desaturation.3
Patients have shown significant improvement both pre and post-ablation with the usage of both medication and CPAP.1 The most important benefit of CPAP may be the reduction in the frequency of the large negative swings in intra thoracic pressure.
Support for the use of oral appliance therapy in OSA has risen with the recent publication research confirming the positive effect of oral appliance therapy on blood pressure and cardiovascular mortality.5,6 Non-compliant or non-tolerant CPAP patients may benefit from oral appliance therapy.
As a dentist when assessing the position of the mandible during the titration, one of our tools is pulse oximetry. What information can be gained by frequent use of pulse oximetry?
What is most significant when assessing the pulse oximetry? Does the oxygen nadir, the oxygen desaturation index, or the duration of time spent below 90% saturation contribute to the atrial fibrillation? What is the best way to manage these patients?
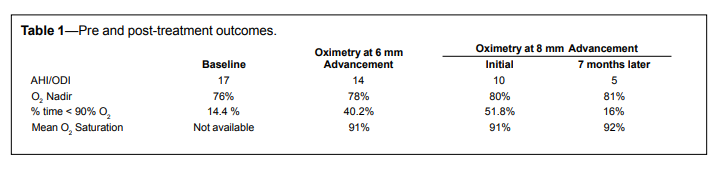
A 66-year-old, overweight (BMI 36.1) male presented with moderate OSA (AHI 17). His medical history included insulin dependent diabetes, hypertension, hypercholesterolemia, and atrial fibrillation. He had cardiac ablation in December 2012. He reported no occurrences of flutter and that he “feels better” since the ablation. He was not able to tolerate CPAP. He was fitted with an oral appliance in April 2013 at an initial advancement of 6 mm of a total protrusive range of 10 mm. Oximetry at the initial setting indicated suboptimal results, and the appliance was advanced to 8 mm and oximetry repeated. Pre- and post-treatment outcomes are shown in Table 1. A second post-treatment oximetry was done 7 months later with no further advancement.
Table 1Pre and post-treatment outcomes. |
{kind=link}
The patient’s cardiologist reviewed the pulse oximetry results, concluding that the reduction in the total number of desaturations was helpful and the hypoventilation related to the obesity was not significant enough to use nocturnal oxygen at this time. As of September 2014, no recurrences of AF have been reported. A follow-up PSG with the appliance in place has been ordered.
Management of these patients might include a log of the time and circumstances of arrhythmic episodes. Aggressive advancement of the mandible to 60% to 70% of protrusion, and close communication with the patient at biweekly intervals may allow for more rapid reduction in symptoms. Regular nocturnal monitoring with pulse oximetry at different points of titration, and frequent communication with the cardiologist helps to improve outcomes. Patients are very grateful when they can finally sleep without the disruption of the atrial fibrillation episode.
Follow-up overnight PSG with the appliance in place after the airway is maximized is critical to determine the effectiveness.
REFERENCES
2. Digby GC, Baranchuk A. Sleep apnea and atrial fibrillation; 2012 update. Curr Cardiol Rev 2012;8:265-72.
3. Vanderveken OM, Boudewyns A, Ni Q, et al. Cardiovascular implications in the treatment of obstructive sleep apnea. J Cardiovasc Transl Res 2011;4:53-60.
4. Ng CY, Liu T, Shehata M, Stevens S, Chugh SS, Wang X. Meta-analysis of obstructive sleep apnea as predictor of atrial fibrillation recurrence after catheter ablation. Am J Cardiol 2011;108:47-51.
5. Phillips CL, Grunstein RR, Darendeliler MA, et al. Health outcomes of continuous positive airway pressure versus oral appliance treatment for obstructive sleep apnea: a randomized controlled trial. Am J Respir Crit Care Med 2013;187:879-87.
6. Anandam A, Patil M, Akinnusi M, Jaoude P, El-Solh AA. Cardiovascular mortality in obstructive sleep apnoea treated with continuous positive airway pressure or oral appliance: an observational study. Respirology 2013;18:1184-90.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September, 2014
Accepted for publication September, 2014
Address correspondence to: Kathleen M. Bennett, DDS, UC Health Medical Arts Bldg., 222 Piedmont Ave., Suite 8300, Cincinnati OH 45219; Tel: (513) 871-9111; Fax: (513) 467-0943; E-mail: kmbennettdds@gmail.com
DISCLOSURE STATEMENT
Dr. Bennett has indicated no financial conflicts of interest.
PDF