Case Report 1, Issue 12.2
Critical Importance of Orofacial Myofunctional Therapy and Surgical Technique in Frenectomy for OSA – A Clinical Case Report
http://dx.doi.org/10.15331/jdsm.7388
Enoch Ng, DDS1,2, Kristin Weaver, RDH, COM3*, Reena Talwar, DDS, PhD2,4
1 Enjoy Dental, Edmonton, Alberta, Canada, 2 School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, 11405-87 Avenue, Edmonton, Alberta, Canada, 3* Harmony Myofunctional Therapy, Alberta, Canada, 4 Contours Oral Surgery, Edmonton, Alberta, Canada
Abstract:
This case report describes the complete resolution of severe obstructive sleep apnea (OSA) in an adult patient through combined orofacial myofunctional therapy (OMT) with lingual frenectomy confirmed through posttreatment home sleep testing. This patient initially underwent a surgically questionable frenectomy without appropriate pretreatment of OMT, leading to worsening OSA. OMT with appropriate frenectomy resulted not only in improvement but also in complete resolution of the patient’s OSA. The importance of appropriate surgical technique for lingual frenectomy is emphasized, with the consequences of poorly performed lingual frenectomy and its effects on the patient’s OSA reviewed in the initial presentation of the patient prior to beginning appropriate OMT.
Keywords:
orofacial myofunctional therapy, lingual frenectomy, obstructive sleep apnea
Citation:
Ng E, Weaver K, Talwar R. Critical Importance of Orofacial Myofunctional Therapy and Surgical Technique in Frenectomy for OSA – A Clinical Case Report. J Dent Sleep Med. 2025;12(2)
INTRODUCTION
Sleep-disordered breathing affects approximately 15% of the population and is characterized by interruptions to breathing during sleep.1-3 Of the sleep breathing disorders, obstructive sleep apnea (OSA) is one of the most common and well known and is well correlated with multiple other medical conditions including diabetes, Alzheimer disease, hypertension, and cardiovascular disease as well as other related symptoms including daytime sleepiness, snoring, and morning headache.4-7 Current recommended primary treatments by the American Academy of Sleep Medicine for OSA include positive airway pressure (PAP) therapy, behavioral strategies (such as weight loss, positional therapy, and avoidance of alcohol and sedatives prior to sleep), oral appliance therapy (OAT), and surgical interventions.8 Other adjunctive treatments include bariatric surgery, pharmacologic/drug treatments, and orofacial myofunctional therapy (OMT).8
OMT has been shown to be effective at helping in the management of OSA in both adults and children, with no risk of negative side effects.9-12 OMT alone has also been shown to reduce OSA index severity by approximately 50% and to improve daytime sleepiness and decrease snoring in adults.12 However, because OMT requires appropriate tongue mobility, lingual ankyloglossia may be an impediment in OMT delivery or achieving the goals of OMT, such as appropriate tongue-jaw dissociation and proper eating, swallowing, and oral rest posture.13-17 Therefore, in certain cases appropriate frenectomy may be necessary to achieve optimal oral function for OMT.17,18
This case report will demonstrate the use of OMT and lingual frenectomy as a treatment for an adult patient with severe OSA, without the requirement for any additional treatments. This case report directly shows correlation between worsening tongue range of motion and increase in apnea-hypopnea index (AHI) from unfavorable healing after initial lingual frenectomy surgery performed without pre-surgical and postsurgical OMT and a comparative decrease in AHI after OMT and lingual frenectomy revision surgery with improved tongue range of motion. One-year follow-up sleep tests will show maintenance of the complete resolution of the patient’s severe OSA.
CASE REPORT
Initial Presentation
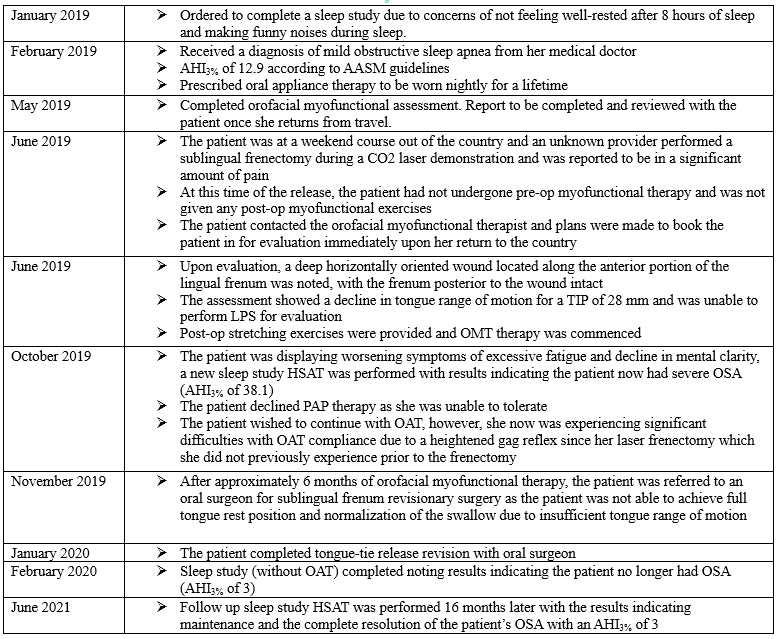
A 61-year-old female patient employed as a dental hygienist presented to a private OMT clinic for an orofacial myofunctional assessment and consultation with “concerns of tethered oral tissue of [the] sublingual frenum”. The patient was evaluated by a certified myofunctional therapist. The patient’s medical history was significant for mild OSA (AHI 12.9), which had been diagnosed 4 months prior to the initial orofacial myofunctional consultation through a home sleep apnea test (HSAT) administered by a sleep physician and was being managed with OAT. Follow-up HSAT for OAT had not yet been conducted. Reported OSA symptoms at the time of assessment included making funny noises during sleep and not feeling well rested from sleep. The patient’s surgical history was significant for tonsil removal when she was 8 years old and previous dental surgery for third molar extraction. The patient reported no current use of medications, no known allergies, and current use of bioderived hormonal supplements.
General physical assessment of the patient revealed a height of 5’10”, weight of 170 lb, neck circumference of 13.5”, and waist circumference of 36”. The patient presented with a forward neck posture, shoulder cant with the right shoulder lower than the left, and a dolichocephalic facial form with an orthognathic profile and normal nasolabial angle.
General dental assessment showed the patient in permanent dentition in Angle class I molar occlusion, incisal overjet of 2.5 mm, incisal overbite of 60%, both maxillary and mandibular midlines approximately 1.5 mm to the right of the facial midline, a V-shaped palatal form with a moderate palatal vault and mild definition of the palatal rugae (Figure 1). Temporomandibular assessment showed mandibular deviation without correction toward the left, no clicking/popping/crepitus, and no reported pain on palpation.
Orofacial myofunctional assessments were conducted to evaluate oral frenal attachments, tongue posture and function, mastication, and swallow functions. Lingual frenal assessment showed the patient with a thin and fibrous sublingual frenum attaching along the ventral midline of the tongue 12 mm from the tongue tip and extending along the floor of the mouth and inserting posterior to the Wharton ducts. Mandibular maximum opening was 51 mm, from which tongue range of motion ratio (TRMR) was then calculated. Maximum opening with tongue tip to incisive papillae (TIP) was 31 mm (61% of maximum mandibular opening with floor of mouth elevation, class 2 TRMR-TIP and considered within normal range of motion) and maximum opening with tongue lingual palatal suction (LPS) was 21 mm (41% of maximum mandibular opening, class 1 TRMR-LPS and considered within normal range of motion if no compensations are present) (Figure 1). Poor tongue-jaw dissociation, weak and limited suction, anterior thrust swallow pattern with facial engagement, and lip weakness were noted. The patient self-reported her tongue rest position as the anterior one-third of the tongue on the palate with the tongue tip to the “spot” and the rest of the tongue low to the floor of the mouth, which denotes a nonideal tongue rest position. The patient underwent oropharyngeal screening, which revealed a Mallampati score of 3, bilateral grade 0 tonsils, and weak palatal velum with prompts.
Prior to the patient beginning OMT, she underwent a CO2 laser lingual frenectomy with an unknown provider during a weekend conference held in a foreign country; postoperative myofunctional exercises were not performed or prescribed. The patient reported experiencing significant pain after the frenectomy and was seen for evaluation with an orofacial myologist immediately upon her return to the country. A deep horizontally oriented wound located along the anterior portion of the lingual frenum was noted, with the frenum posterior to the wound intact (Figure 2). The assessment showed a decline in tongue range of motion for a TRMR-TIP of 28 mm and the patient was unable to perform LPS for evaluation. Postcare exercises and instructions were provided to the patient along with concerns related to scar tissue formation potentially worsening the tongue’s range of motion. OMT was continued through the healing process to help rehabilitate muscle strength and optimize oral function. Because of symptoms of excessive fatigue and decline in mental clarity, a new sleep study was performed with results indicating the patient now had severe OSA (AHI 38.1). Six months after the frenectomy was performed, a reevaluation was conducted to assess the need for revisionary surgery. Assessment after complete wound healing showed scar tissue with significant deficiencies in tongue mobility with a TRMR-TIP of 25 mm and a TRMR-LPS of 24 mm. The patient was not able to achieve full tongue rest position. The patient also was unable to achieve normalization of the swallow because of insufficient tongue range of motion specific to mid-tongue elevation to seal for lingual palatal swallow. Despite her new diagnosis and even after discussions with her sleep physician, the patient declined PAP therapy noting she was unable to tolerate it and wished to continue with OAT. However, the patient also reported significant difficulties with OAT compliance because of a heightened gag reflex since her laser frenectomy, which the patient reported as not previously experiencing prior to the frenectomy. The patient was also insistent on proceeding with OMT if at all possible.
After reevaluation and education that a frenectomy revision surgery may be necessary to optimize her OMT results, the patient agreed to proceed with OMT.
In-person OMT sessions were provided on a biweekly basis, with orofacial myofunctional activities directed at strengthening and improving muscle coordination for normalized eating, chewing, swallowing, and resting patterns. Orofacial myofunctional treatment goals included nasal breathing during the day and night, lips closed at rest with no facial strain, tongue fully resting on the palate at rest, proper eating, chewing, and swallowing. Orofacial myofunctional activities were introduced to strengthen the velum, genioglossus, palatoglossus, styloglossus, and orbicularis oris. Establishing correct intraoral pressure and lingual palatal suction were essential to enable a normalized lingual palatal swallow and tongue resting position. Lingual functions were established to support organization for eating, chewing, and bolus collection. Compensatory muscles of facial expression were eliminated from use during the swallow. The patient struggled to achieve a normalized swallow pattern and proper tongue rest position. The difficulty was narrowed down to midblade and posterior tongue range-of- motion deficiencies.
Total OMT treatment time prior to lingual ankyloglossia revision surgery was 6 months. Because the primary reason for lingual ankyloglossia release was for myofunctional purposes, no sleep study was ordered. A lingual frenum Z-plasty revision surgery was performed by a board-certified oral maxillofacial surgical specialist with the patient under general anesthesia and without complications for the purposes of increasing tongue range of motion for the improvement of OMT outcomes. OMT was continued post-surgery, with the importance of specific activities targeting the intrinsic and extrinsic muscles of the tongue emphasized. Total treatment time of postsurgical OMT was extended to 9 months because of COVID-19 disrupting regular appointments, at which point the patient showed maximization of oral muscular movement and normalization of eating, chewing, swallowing, and rest posture. The patient’s maximum mandibular opening was 53 mm, tongue range of motion TIP measurement was 48 mm (90% of maximum opening), and LPS was 29 mm (54% of maximum opening). The patient reported her tongue rest position was fully along the palate up until the soft palate. Based on the patient’s oral motor function improvements and a reported increase in weight of 20 lb, a new HSAT was performed without use of the dental appliance from OAT, for which the patient reported significant continued compliance difficulties, with results indicating the patient now no longer had OSA (AHI 3). Following this HSAT result, the patient discontinued OAT. A follow-up HSAT was performed 16 months later, with the results indicating maintenance and the complete resolution of the patient’s OSA, with an AHI of 3.
Figure 1:Intraoral photographs of the patient’s mouth pretreatment, showing occlusion and tongue range of motion. |
{kind=link}
{kind=link}
Supplemental Table |
{kind=link}
DISCUSSION
Current guidelines recommend that the primary treatment for OSA is PAP therapy, with alternative treatments including behavioral strategies, OAT, and surgical interventions.8 However, there are significant limitations with these treatments, including patients declining and/or discontinuing these treatment options due to discomfort, fear of negative side effects, lack of compliance, lack of efficacy for the treatment of severe OSA, and associated risks with treatments (such as surgical risks, including from having OSA).8,19-27
Although previous research has shown that OMT does not provide complete resolution of OSA, this case report shows that OMT in combination with lingual ankyloglossia released through frenectomy may be an appropriate treatment option for patients who otherwise forgo primary treatment options for OSA, especially in patients with a restrictive lingual frenum either naturally or from previous lingual frenectomy surgery.12 Patients with residual restrictive frenums or worsening range of motion from inappropriate surgical technique and lack of coordinated OMT may particularly benefit from this type of corrective therapy. However, this case report also shows the importance of tongue function and the effect that lingual frenal restrictions can have on patients with OSA. This may be particularly important for patients with a phenotypic presentation of OSA predominated by tongue base collapse, as increased tongue range of motion from lingual frenectomy with improved neuromuscular tone from OMT may directly address this component of OSA.28,29 As shown in this case report, inappropriate use of lingual frenectomy can have significant negative consequences for patients that may not be otherwise considered by either professionals who perform this procedure or by patients seeking frenectomy for lingual ankyloglossia. This is in agreement with previous published research on infants and children on the importance of surgical technique for frenectomies and the effect of restrictive lingual frenums on pediatric OSA, and that appropriately conducted frenectomies with OMT can significantly improve signs and symptoms of OSA in adults.30-34 Appropriate training prior to providing any frenectomy surgery and interdisciplinary collaboration to ensure appropriate preoperative and postoperative OMT are of vital importance when performing a frenectomy in both children and adults, especially for patients for whom services are being provided specifically to address OSA.
CONCLUSION
This case report shows the successful combined use of OMT and lingual frenectomy as a comprehensive treatment for a patient with severe OSA. This case report also emphasizes the importance of proper surgical technique for lingual frenectomy, which if done inappropriately can significantly worsen a patient’s OSA. Further research into the combination of OMT and lingual frenectomy is necessary to determine appropriate patient selection criteria, delivery methodology, and generalizability to patients with OSA who cannot tolerate or who decline primary OSA treatment options.
ACKNOWLEGEMENT
The authors would like to thank Dr. Tammarie Heit (Avalon Dental, Edmonton, Alberta, Canada) for overseeing the dental sleep appliance care of the patient during OMT.
ABBREVIATIONS
AHI: apnea-hypopnea index
HSAT: home sleep apnea test
LPS: lingual palatal suction
OAT: oral appliance therapy
OMT: orofacial myofunctional therapy
OSA: obstructive sleep apnea
PAP: positive airway pressure
TIP: tongue to incisive papilla
TRMR: tongue range of motion ratio
REFERENCES
- Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311-1322. doi: 10.3978/j.issn.2072-1439.2015.06.11.
- Frost & Sullivan. Hidden health crisis costing America billions. American Academy of Sleep Medicine. 2016. Available at: https://aasm.org/advocacy/initiatives/economic-impact-obstructive-sleep-apnea/. Accessed January 21, 2021.
- Frost & Sullivan. In an age of constant activity, the solution to improving the nation’s health may lie in helping it sleep better. American Academy of Sleep Medicine. 2016. Available at: https://aasm.org/advocacy/initiatives/economic-impact-obstructive-sleep-apnea/. Accessed January 21, 2021.
- Anker SD, von Haehling S, Germany R. Sleep-disordered breathing and cardiovascular disease. Indian Heart J. 2016;68(Suppl 1):S69-S76. doi: 10.1016/j.ihj.2015.11.018.
- Wang X, Bi Y, Zhang Q, Pan F. Obstructive sleep apnoea and the risk of type 2 diabetes: A meta-analysis of prospective cohort studies. Respirology. 2013;18(1):140-146. doi: 10.1111/j.1440-1843.2012.02267.x.
- Gami AS, Howard DE, Olson EJ, Somers VK. Day-night pattern of sudden death in obstructive sleep apnea. N Engl J Med. 2005;352(12):1206-1214. doi: 10.1056/NEJMoa041832.
- Young T, Finn L, Peppard PE, et al. Sleep disordered breathing and mortality: Eighteen-year follow-up of the Wisconsin sleep cohort. Sleep. 2008;31(8):1071-1078.
- Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263-276.
- Guilleminault C, Huang YS, Monteyrol PJ, Sato R, Quo S, Lin CH. Critical role of myofascial reeducation in pediatric sleep-disordered breathing. Sleep Med. 2013;14(6):518-525. doi: 10.1016/j.sleep.2013.01.013.
- Guilleminault C, Huang YS. From oral facial dysfunction to dysmorphism and the onset of pediatric OSA. Sleep Med Rev. 2018;40:203-214. doi: 10.1016/j.smrv.2017.06.008.
- Huang YS, Hsu SC, Guilleminault C, Chuang LC. Myofunctional therapy: Role in pediatric OSA. Sleep Med Clin. 2019;14(1):135-142. doi: 10.1016/j.jsmc.2018.10.004.
- Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: A systematic review and meta-analysis. Sleep. 2015;38(5):669-675. doi: 10.5665/sleep.4652.
- Chinnadurai S, Francis DO, Epstein RA, Morad A, Kohanim S, McPheeters M. Treatment of ankyloglossia for reasons other than breastfeeding: A systematic review. Pediatrics. 2015 Jun;135(6):e1467-74. doi: 10.1542/peds.2015-0660.
- Stecco C. Functional Atlas of the Human Fascial System. Churchill Livingstone; 2014.
- Yoon A, Zaghi S, Weitzman R, et al. Toward a functional definition of ankyloglossia: Validating current grading scales for lingual frenulum length and tongue mobility in 1052 subjects. Sleep Breath. 2017;21(3):767-775. doi: 10.1007/s11325-016-1452-7.
- Gross AM, Kellum GD, Hale ST, et al. Myofunctional and dentofacial relationships in second grade children. Angle Orthod. 1990;60(4):247-253; discussion 254. doi: 10.1043/0003-3219(1990)060<0247:MADRIS>2.0.CO;2.
- Oral rest posture: A key piece of the obstructive sleep apnea puzzle. Sleep Review: Web Edition Articles (USA). 2016. Available at: https://sleepreviewmag.com/curated/oral-rest-posture-key-piece-of-obstructive-sleep-apnea-puzzle/ Accessed August 15, 2021.
- Zaghi S, ValcuâPinkerton S, Jabara M, et al. Lingual frenuloplasty with myofunctional therapy: Exploring safety and efficacy in 348 cases. Laryngoscope Investig Otolaryngol. 2019;4(5):489-496. doi: 10.1002/lio2.297.
- Sutherland K, Phillips CL, Cistulli PA. Efficacy versus effectiveness in the treatment of obstructive sleep apnea: CPAP and oral appliances. J Dent Sleep Med. 2015;2(4):175-181. doi: 10.15331/jdsm.5120.
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11(7):773-827. doi: 10.5664/jcsm.4858.
- Vasu TS, Grewal R, Doghramji K. Obstructive sleep apnea syndrome and perioperative complications: A systematic review of the literature. J Clin Sleep Med. 2012;8(2):199-207. doi: 10.5664/jcsm.1784.
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: Occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291. doi: 10.5664/jcsm.4278.
- Sanders AE, Essick GK, Fillingim R, et al. Sleep apnea symptoms and risk of temporomandibular disorder: OPPERA cohort. J Dent Res. 2013;92(Suppl 7):70S-77S. doi: 10.1177/0022034513488140.
- Perez CV, de Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2013;17(1):323-332. doi: 10.1007/s11325-012-0695-1.
- Sheats R, Schell T, Blanton A, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;4(4):111-125. doi: 10.15331/jdsm.6746.
- Almeida FR, Henrich N, Marra C, et al. Patient preferences and experiences of CPAP and oral appliances for the treatment of obstructive sleep apnea: A qualitative analysis. Sleep Breath. 2013;17(2):659-666. doi: 10.1007/s11325-012-0739-6.
- Choi J-A, Yoon I-Y, Han E-G, Lee S. Subjective and objective CPAP compliance in patients with obstructive sleep apnea syndrome. Sleep Med Res. 2011;2(2):63-68. doi: 10.17241/smr.2011.2.2.63.
- Vroegop AV, Vanderveken OM, Boudewyns AN, et al. Drug-induced sleep endoscopy in sleep-disordered breathing: report on 1,249 cases. Laryngoscope. 2014;124(3):797-802. doi:10.1002/lary.24479
- Eckert DJ. Phenotypic approaches to obstructive sleep apnoea - New pathways for targeted therapy. Sleep Med Rev. 2018;37:45-59. doi:10.1016/j.smrv.2016.12.003
- Solis-Pazmino P, Kim GS, Lincango-Naranjo E, Prokop L, Ponce OJ, Truong MT. Major complications after tongue-tie release: A case report and systematic review. Int J Pediatr Otorhinolaryngol. 2020;138:110356. doi:10.1016/j.ijporl.2020.110356
- Govardhan C, Murdock J, Norouz-Knutsen L, Valcu-Pinkerton S, Zaghi S. Lingual and maxillary labial frenuloplasty with myofunctional therapy as a treatment for mouth breathing and snoring. Case Rep Otolaryngol. 2019;2019:3408053. Published 2019 Mar 10. doi:10.1155/2019/3408053
- Bussi MT, Corrêa CC, Cassettari AJ, et al. Is ankyloglossia associated with obstructive sleep apnea? [published online ahead of print, 2021 Nov 5]. Braz J Otorhinolaryngol. 2021;S1808-8694(21)00181-6. doi:10.1016/j.bjorl.2021.09.008
- Fioravanti M, Zara F, Vozza I, Polimeni A, Sfasciotti GL. The efficacy of lingual laser frenectomy in oediatric OSAS: A randomized double-blinded and controlled clinical study. Int J Environ Res Public Health. 2021;18(11):6112. Published 2021 Jun 6. doi:10.3390/ijerph18116112
- Zaghi S, Valcu-Pinkerton S, Jabara M, et al. Lingual frenuloplasty with myofunctional therapy: Exploring safety and efficacy in 348 cases. Laryngoscope Investig Otolaryngol. 2019;4(5):489-496. Published 2019 Aug 26. doi:10.1002/lio2.297
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted April 4, 2022
Submitted in final revised form July 8, 2024
Accepted for publication August 26, 2024
Address correspondence to: Kristin Weaver, RDH, COM, Harmony Myofunctional Therapy, 33 Tuscany Meadows Common NW, Calgary Alberta, T3L 2L3.
Email: harmonymyotherapy@gmail.com.
DISCLOSURE STATEMENT
The authors have no conflicts of interest to declare.
PDF