Case Report 1, Issue 12.1
Consequences and Implications of Discontinuing Oral Appliance Therapy for Obstructive Sleep Apnea: Be True to the Tooth
http://dx.doi.org/10.15331/jdsm.7374Hitoshi Taga, DDS, PhD1,2, Tatsuya Fukuda, DDS3,4, Haruto Katahira, DDS, PhD5, Miiko Taga, DDS1, Satoru Tsuiki, DDS, PhD3,4
1 Taga Dental Clinic, Tokyo, Japan; 2 JR Tokyo General Hospital, Tokyo, Japan; 3 Institute of Neuropsychiatry, Tokyo, Japan; 4 Fukuda Dental and Orthodontic Clinic, Tokyo, Japan; 5 Katahira Dental Clinic, Tokyo, Japan
ABSTRACT
Sustained direct pressure on the teeth applied by wearing a mandibular advancement device (MAD) would lead to unwanted tooth movement and occlusal changes in oral appliance therapy for obstructive sleep apnea (OSA). When the observed occlusal changes are rather serious, it is an appropriate decision for sleep dentists/physicians to propose that such patients discontinue MAD use and to offer a substitute to continue managing OSA. Both orthodontic treatment and continuous positive airway pressure (CPAP) therapy appear to be promising approaches to addressing such an unfavorable dental consequence, and offer an alternative to MAD. However, compared with teenage orthodontic patients and treatment-naïve individuals with OSA, it is noteworthy that orthodontic treatment and CPAP therapy for elderly patients who discontinue MAD use are likely to clinically involve more risks and difficulties, which would consequently affect prognosis of each treatment. Moreover, most patients who discontinued MAD use are rarely indicated for surgical procedures or hypoglossal nerve stimulation therapy. Although the tongue-retaining device is currently not assumed as an option of OSA treatment, renovation of this device and/or innovation of devices to minimize or avoid known dental adverse effects of both MADs and CPAP will be an adequate future direction of patient-centered OSA treatment.
Keywords:
obstructive sleep apnea, dental side effects, mandibular advancement device, continuous positive airway pressure, orthodontic treatment
Citation:
Taga H, Fukuda T, Katahira H, Taga M, Tsuiki S. Consequences and implications of discontinuing oral appliance therapy for obstructive sleep apnea: Be true to the tooth. J Dent Sleep Med. 2025;12(1)
INTRODUCTION
Mandibular advancement devices (MADs) are a common treatment for obstructive sleep apnea (OSA). However, long-term use can lead to complications, including tooth movement and changes in occlusion. These adverse effects, such as difficulty biting or chewing, can be upsetting for patients, especially when discontinuation of MAD use is advised. Sustained pressure from MADs can cause irreversible dental changes, necessitating alternative treatments such as orthodontics or continuous positive airway pressure (CPAP) therapy.1-2 For elderly patients, these options can involve greater risks and complexities, affecting treatment prognosis. This article discusses the challenges and clinical considerations in transitioning from MAD therapy to alternative treatments.
Treatment involved initiating CPAP therapy in concert with orthodontic correction using a fixed edgewise appliance. After 1 year and 7 months of active orthodontic treatment, malocclusion was resolved. The patient was provided with retainers to maintain the corrected occlusion and encouraged to continue CPAP use.
CASE REPORT
A 63-year-old man with mild OSA (baseline apnea-hypopnea index = 13.3/hour, body mass index = 22.1 kg/m²) presented with complaints of chewing difficulty after 8 years of MAD use. Despite good adherence to therapy (average >4 hours/night, 5 days/week), clinical evaluation revealed few occlusal contacts and significant malocclusion. The patient's OSA had progressed to moderate severity (apnea-hypopnea index = 21.9/hour), as confirmed by a follow-up polysomnographic study after discontinuing MAD use.
Figures 1. Malocclusion and corrected occlusion.Left, Initial presentation of malocclusion with anterior and lateral crossbite due to mandibular advancement device use in a patient age 63 years, 6 months. |
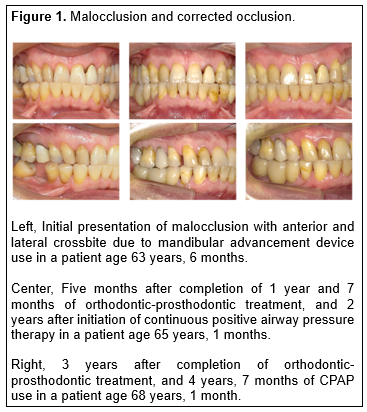{kind=link}
DISCUSSION
- Risks of Long-Term MAD Use
- Sustained pressure on teeth increases the likelihood of severe occlusal changes, especially in compliant users.
- Early collaboration between sleep dentists and orthodontists may mitigate risks.
- Mild morning occlusal shifts could signal irreversible changes, necessitating proactive intervention.1,2
- Transition to CPAP Therapy
- Although CPAP effectively manages OSA, patient adherence can be challenging. Acceptance of CPAP may be lower in patients transitioning from MAD therapy.
- Costs for CPAP and orthodontic treatment can be substantial, especially in countries where reimbursement policies are restrictive. For instance, orthodontic treatment in Japan ranges from 800,000 to 1.2 million yen (approximately $5,500–$8,300 USD).3
- Potential Complications
- CPAP use may lead to anterior crossbite due to sustained pressure on upper incisors or tongue movement.4
- In the reported case, minor incisor movement was observed, but no significant complications arose.
- Reusing MADs after orthodontic treatment risks relapse into malocclusion.
- Future Directions
- Noninvasive alternatives to MADs and CPAP, such as tongue-retaining devices or innovative therapies, are needed to minimize dental adverse effects.5,6
- Patient-centered designs that address individual anatomic and functional needs could improve outcomes and adherence.
CONCLUSION
Discontinuing MAD use and transitioning to CPAP therapy is a viable but complex path, requiring careful consideration of patient-specific factors. For older patients with compromised dentition, orthodontic treatment may involve extended retention periods. Innovation in OSA treatment devices is crucial to reduce adverse effects and enhance patient care. Studies performed within dental schools are fundamental to assessing the extent of knowledge and awareness of dental students, identifying specific gaps, and implementing the corresponding educational contents accordingly. By doing so, dental schools can better equip future dental providers with the necessary knowledge and skills to identify, manage, and collaborate effectively in the treatment of patients with OSA.
REFERENCES
- Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: An update for 2015. J Clin Sleep Med. 2015;11(7):773-827. doi: 10.5664/jcsm.4858.
- Behrents RG, Shelgikar AV, Conley RS, et al. Obstructive sleep apnea and orthodontics: An American Association of Orthodontists White Paper. Am J Orthod Dentofacial Orthop. 2019;156(1):13-28.e1. doi: 10.1016/j.ajodo.2019.04.009.
- About orthodontic treatment. Japanese Orthodontic Society. Accessed December 13, 2024. https://www.jos.gr.jp/about
- Pliska BT, Almeida FR. Tooth movement associated with CPAP therapy. J Clin Sleep Med. 2018;14(4):701-702.
- Yanagihara M, Tsuiki S, Setoguchi Y, Inoue Y. Treatment of obstructive sleep apnea with a tongue-stabilizing device at a single multidisciplinary sleep center. J Dent Sleep Med. 2016;3(2):43–47.
- Fukuda T, Takei Y, Nakayama H, Inoue Y, Tsuiki S. Continuous tongue suction as a potential therapy for obstructive sleep apnea: A feasibility study. J Dent Sleep Med. 2020;7(3). http://dx.doi.org/10.15331/jdsm.6746
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted August 7, 2024
Accepted for publication December 9, 2024
Address correspondence to: Satoru Tsuiki, DDS, PhD, Research Department, Institute of Neuropsychiatry, 91, Bentencho, Shinjuku-ku, Tokyo 162-0851, Japan. Email: strtsuiki@gmail.com.