Case Report 1, Issue 1.1
Effects of the Association of nCPAP and Tongue Positioner Device in OSAS Treatment: A Case Report
http://dx.doi.org/10.15331/jdsm.3732
Domenico Ciavarella, DDS1 ; Roberto Sabato, MD2 ; Giovanni Battista, DDS1 ; Lorenzo Lo Muzio, MD, DDS1 ; Giuseppina Campisi, DDS3 ; Michele Cassano, MD1 ; Lucio Lo Russo, DDS, PhD1 ; Maria Pia Foschino Barbaro, MD2
1 Department of Clinical and Experimental Medicine, Faculty of Medicine, School of Dentistry, University of Foggia, Foggia, Italy; 2 Department of Medical and Surgical Sciences, Faculty of Medicine, University of Foggia, Foggia, Italy; 3 Department of Surgical and Oncological Disciplines, V. Margiotta Oral Medicine Unit, Palermo University Hospital, Palermo, Italy
ABSTRACT
Study Objectives:
Obstructive sleep apnea syndrome (OSAS) is a common disorder in middle-aged people associated with increased cardiovascular and cerebrovascular morbidity and mortality, excessive daytime somnolence, and impaired daytime cognitive function. Its management includes removal of risk factors (if feasible), nasal continuous positive airway pressure (nCPAP), surgical treatment (usually, reserved for cases in whom nCPAP failed), and, in non-severe cases, the application of oral appliances (mandible-advancement devices [MAD] or tongue positioner devices [TPD]). The beneficial effect of the association of TPD with nCPAP was investigated.
Design:
TPD associated with nCPAP was compared to other approaches: i.e., MAD, TPD alone, nCPAP alone.
Patients:
A 55-year-old man with moderate OSAS and a retrusive position of the mandible and the tongue.
Interventions:
series of polysomnographies and cephalometric evaluation.
Measurements and Results:
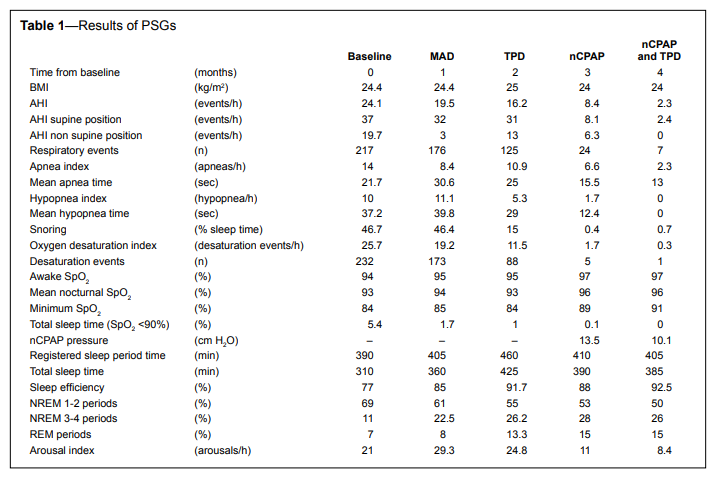
baseline parameters were: AHI (apnea-hypopnea index) 24.1 events/h, with 127 episodes of apnea (mean apnea period: 21.7 s), 90 episodes of hypopnea (mean hypopnea period: 37.2 s) and oxygen saturation (SpO2 %) between 84% and 94%. The best improvements were obtained with nCPAP associated with TPD: AHI 2.3 events/h, 7 episodes of apnea (mean apnea period: 13 s), and SpO2 % between 91% and 97%.
Conclusions:
the association between TPD, which helps in opening the upper airway space, and nCPAP may significantly improve nighttime respiratory function and sleep efficiency using lower nCPAP pressure.
Keywords:
obstructive sleep apnea syndrome, oral appliances, CPAP, cephalometry, tongue position
Citation:
Ciavarella D, Sabato R, Battista G, Lo Muzio L, Campisi G, Cassano M, Lo Russo L, Foschino Barbaro MP. Effects of the association of nCPAP and tongue positioner device in OSAS treatment: a case report. Journal of Dental Sleep Medicine 2014;1(1):21–23.
Obstructive sleep apnea syndrome (OSAS) is a common disorder in middle-aged people (30-60 years), affecting 4% of men and 2% of women. OSAS may be associated with increased cardiovascular and cerebrovascular morbidity and mortality,1 excessive daytime somnolence, and impaired daytime cognitive function, which may be recognized as a cofactor in the etiology of road traffic accidents.2
OSAS management includes removal of risk factors, if feasible, nasal continuous positive airway pressure (nCPAP), surgical treatment (usually, reserved for cases in whom nCPAP failed)3 and, in non-severe cases, the application of oral appliances (mandible-advancement devices [MAD] or tongue positioner devices [TPD])4 .
In the present paper, the beneficial effect of the association of TPD with nCPAP in a moderate case of OSAS with a retrusive position of the mandible and the tongue.
REPORT OF CASE
A 55-year-old man with no sleep-related breathing disorders (SRBD) risk factors (e.g., obesity, increased neck circumference, anatomical abnormalities of the face5 ) experiencing daytime sleepiness, snoring and waking up at night was evaluated in the sleep laboratory of Respiratory Diseases center of the University of Foggia. The patient was continuously monitored in one night using a portable device (Embletta, Flaga, Reykjavik, Iceland).6 Recordings included airflow (by placing a nasal cannula at the nose and at the mouth, and by oro-nasal thermistor); snoring (by a microphone placed at the neck); ECG; sleep position; thoracic-abdominal movements (detected through 2 piezoelectric belts); overnight oxygen saturation (by finger pulseoximetry); electroencephalographic, electro-oculographic, and chin electromyographic recordings (by means of surface electrodes according to the international 10-20 electrode placement system for sleep).
Results from the baseline polysomnography (PSG) analysis are shown in Table 1. Briefly, an AHI of 24.1 events/h was calculated, with 127 episodes of apnea (mean apnea period: 21.7 s), 90 episodes of hypopnea (mean hypopnea period: 37.2 s) and oxygen saturation (SpO2 %) between 84% and 94%. The diagnosis of moderate OSAS was made and the patient referred to the School of Dentistry of the University of Foggia for evaluation of intra- and extra-oral conditions associated with SRBD. Cephalometric evaluation, made on a lateral-head x-ray film, revealed a severe maxillary and mandibular retrusive position with a large tongue.
Table 1Results of PSGs |
{kind=link}
A MAD (Figure 1A-C) consisting of 2 acrylic splints capable to reposition the mandible 4 mm forward (measured with a George gauge from the tip of central inferior incisors with the mandible in resting position) was fabricated and the patient instructed to wear it for one month. Then, a second lateral head film and a PSG were performed (Table 1); since many apnea events were still present, another oral appliance, i.e., TPD (AveoTSD) (Figure 1D-E) was used and results re-evaluated one month later with a new PSG. After, nCPAP treatment, with a self-adjusting device (Auto-CPAP, RES MED S9), was performed and evaluated with a PSG: an AHI of 8.4 events/h was calculated, with 19 episodes of apnea (mean apnea period: 15.5 s), 5 episodes of hypopnea (mean hypopnea period: 12.4 s) and SpO2 % between 89% and 97%. Although AHI was greatly improved, the overall results were not deemed satisfactory; thus, a course of nCPAP associated with TPD was performed (Figure 1H, I); this provided the best results on nights respiratory function, sleep efficiency, and oxygen saturation, using a lower nCPAP pressure.
Figure 1 |
{kind=link}
DISCUSSION
In the present paper, a patient with a retrusive mandibular position, closure of upper airway space, and moderate/severe OSAS who refused surgical treatment was treated with various approaches.Recently, MADs and TPDs have received great interest as low-cost strategies for treatment of obstructive OSAS.7 In fact, the anterior mandible and tongue repositioning causes complex changes within the lateral pharyngeal walls, tongue, soft palate, epiglottis, and genioglossus muscle that induce an improvement of respiratory dynamics.8 However, minor (tooth pain, excess salivation, dry mouth, TMJ discomfort, and muscle pain) and severe complications (TMJ dysfunction, gagging, tooth movement, intractable muscle pain) are possible. Thus, adequate selection of patients is mandatory. Oral appliances are indicated and may succeed in non-severe OSAS. Based on the present case, oral appliances may also have a beneficial effect in moderate-severe obstructive cases in conjunction with nCPAP. In fact, the latter still remains the golden standard for such cases, but whenever a retrusive position of mandible and/ or the tongue is present, posterior airway space may be affected, possibly reducing nCPAP effectiveness. Our results confirm that in such a case the association between TPD, which helps in opening the upper airway space, and nCPAP may significantly improve nighttime respiratory function and sleep efficiency using lower nCPAP pressure.
REFERENCES
2. Sassani A, Findley LJ, Kryger M, Goldlust E, George C, Davidson TM. Reducing motor-vehicle collisions, costs, and fatalities by treating obstructive sleep apnea syndrome. Sleep 2004;27:453-8.
3. Brigance JS, Miyamoto RC, Schilt P, et al. Surgical management of obstructive sleep apnea in infants and young toddlers. Otolaryngol Head Neck Surg 2009;140:912-6.
4. Ciavarella D, Sabatucci A, Mastrovincenzo M, et al. Obstructive sleep apnea treatment with a new oral appliance: Somnodent. Open Othorinolaryngol J 2009;3:34-8.
5. Bliwise DL, Feldman DE, Bliwise NG, et al. Risk factors for sleep disordered breathing in heterogeneous geriatric populations. J Am Geriatr Soc 1987;35:132-41.
6. Dingli K, Coleman EL, Vennelle M, et al. Evaluation of a portable device for diagnosing the sleep apnoea/hypopnoea syndrome. Eur Respir J 2003;21:253-9.
7. Eckhart J. Comparison of oral devices for snoring. CDA J 1998;26:611-23.
8. Moore EK. Oral appliance treatment for obstructive sleep apnea. Oper Tech Otolaryngogl 2007;18:52-6.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication September, 2013
Submitted in final revised form January, 2014
Accepted for publication January, 2014
Address correspondence to: Dr. Domenico Ciavarella, Via Rovelli n.48, 71100 Foggia-Italy; Tel: +39 347 6131225; Fax: +39 0881 588086; E-mail: domenico.ciavarella@unifg.it
DISCLOSURE STATEMENT
This was not an industry supported study. The authors have indicated no financial conflicts of interest.