Case Report 1, Issue 10.3
Passive Orofacial Myofunctional Therapy Appliance for Treating Obstructive Sleep Apnea: A Clinical Case Report
http://dx.doi.org/10.15331/jdsm.7302Enoch T Ng, DDS1, Laura Chan, OD, RN, MSc2
1Clinical Dentist, Enjoy Dental, Edmonton, Alberta, Canada. Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta; 2Optometrist and Registered Nurse in Edmonton, Alberta, Canada
ABSTRACT
Current treatment options for patients with obstructive sleep apnea include continuous positive airway pressure, oral appliance therapy, behavioral management, and adjunctive therapies that include orofacial myofunctional therapy (OMT). Certain dental appliances used for OMT can be worn at night and include components to encourage proper tongue and lip placement, important components in OMT. This case report describes the use of a passive OMT appliance in the successful treatment of a patient with moderate obstructive sleep apnea.
Keywords:
orofacial myofunctional therapy, dental sleep medicine, obstructive sleep apnea
Citation:
Ng ET, Chan L. Passive orofacial myofunctional therapy appliance for treating obstructive sleep apnea: A clinical case report. J Dent Sleep Med. 2023;10(3)
INTRODUCTION
Sleep breathing disorders (SBDs), also known as sleep-disordered breathing, are a group of medical conditions affecting more than 15% of the global population. Although there are many different types of SBDs, upper airway resistance syndrome (UARS) and obstructive sleep apnea (OSA) may be of particular interest to dentists. OSA is characterized by repetitive partial or complete obstructions in the upper airway, usually along the pharyngeal segment, while maintaining the thoracic effort of breathing and with associated oxygen desaturations and/or neurologic arousals. UARS is very similar to OSA but without the oxygen desaturations. For both UARS and OSA, the neuroarousals and intermittent oxygen desaturations have a cascading effect on health and function, with well-established correlations with other chronic conditions including diabetes, hypertension, myocardial infarction, cerebrovascular infarction, dementia, Alzheimer disease, and daytime sleepiness.
For both UARS and OSA, diagnosis is confirmed with a home sleep apnea test (HSAT). Although OSA is defined by an apnea-hypopnea index greater than 5, UARS is traditionally diagnosed when a HSAT is negative for OSA but with respiratory disturbance and the patient is experiencing symptoms of daytime sleepiness and/or fatigue. Both UARS and OSA have the same treatment options; continuous positive airway pressure (CPAP), oral appliance therapy (OAT), surgery, weight loss, behavioral management, and adjunctive therapies such as orofacial myofunctional therapy (OMT).
Orofacial myofunctional disorders (OMDs) are correlated with SBDs, with worse OMDs correlating with increased severity of SBDs.1 OMDs include low tongue posture, lip incompetence, tongue thrust swallow pattern, presence of noxious oral habits, and difficulty with appropriate dissociation of orofacial muscles. OMT used to correct OMDs can result in improvements of up to 50% in patients with OSA.2-4 It is for this reason that OMT is not considered a primary stand-alone treatment for OSA.
Passive OMT appliances (appliances that sit passively in the mouth to aid in OMT, usually to aid specifically in tongue and lip positioning, without components specifically designed for active tooth movement) are a relatively new creation and may provide an interesting treatment option for patients with UARS and mild OSA. Passive OMT appliances encourage a myofunctionally appropriate tongue position and lip competence with minimal mandibular protrusion. Although OAT for OSA has traditionally placed the mandible at 50% of maximum protrusion and titrated the jaw anteriorly, recent research indicates that minimal protrusion may be sufficient.5-7 Minimizing protrusion is important because increased protrusion is correlated with increased risks of adverse effects such as temporomandibular joint dysfunction, long-term changes to craniofacial structure, dental occlusal changes, and other soft-tissue adverse effects.7-10 Although passive OMT appliances are ’stock made (non-custom prefabricated)‘ and not designed to be titratable, recent research indicating minimal protrusion may be sufficient in OAT makes the use of passive OMT appliances a potentially appropriate treatment option for patients with SBDs. This is especially true because the components aiding in appropriate tongue positioning may help manage one of the important anatomic points of collapse in the upper airway: the tongue. This means that passive OMT appliances may provide sufficient therapeutic benefit for some patients with SBDs without the costs associated with custom-fit titratable appliances used in OAT. In addition, there are significantly decreased risks of adverse effects commonly associated with protrusive positioning traditionally used in OAT, and faster treatment delivery because the appliances may be held ‘in stock’ rather than having to be custom made.
This case study describes the use of a passive OMT appliance in the treatment of mild/moderate OSA immediately after an initial sleep study, demonstrating the ability of passive OMT appliances to be used in OAT for quick delivery of care and complete index management.
REPORT OF CASE
A 32-year-old female presented to a dental clinic with a previous diagnosis of OSA by a sleep physician through a home sleep test and with concerns of “tired all the time, yearly colds” and seeking to “feeling rested”. The patient had already declined standard CPAP therapy for OSA. The patient’s primary concerns, in ranked order, were (1) significant daytime sleepiness; (2) frequent heavy snoring; (3) feeling unrefreshed in the morning; (4) back pain; and (5) headaches. The patient reported no medical conditions significant for anemia, asthma, chronic fatigue, poor sleep, muscle aches, minor hearing impairment, or gastroesophageal reflux, and experienced a prolonged urinary tract infection that was resolved several years ago. The patient reported no current medications and/or supplements, though she did report taking acetaminophen or ibuprofen as needed for pain management. The patient reported having a metal (nickel) allergy. The patient reported sleeping on her back and side, no difficulties with falling asleep, difficulties with staying asleep, waking not feeling rested, and chronic mouth breathing. The patient’s Epworth Sleepiness Scale score was 14, Nighttime Sleepiness Evaluation score was 9, STOP-BANG score was 3, and Berlin Questionnaire rating was high risk. Clinical examination showed relatively average mandibular ranges of motion (50 mm maximum opening with a 2 mm left deflection, 8 mm of left and right lateral excursion, and 4 mm of protrusion). The patient had a current dentition status of left and right molar classification of Angle class 3, an overjet of 1 mm, and overbite of 0.5 mm. Based on the collected data, radiographic imaging was performed and findings reviewed by a medical radiologist, who indicated no radiographic findings of significance that would contraindicate the use of dental appliances.
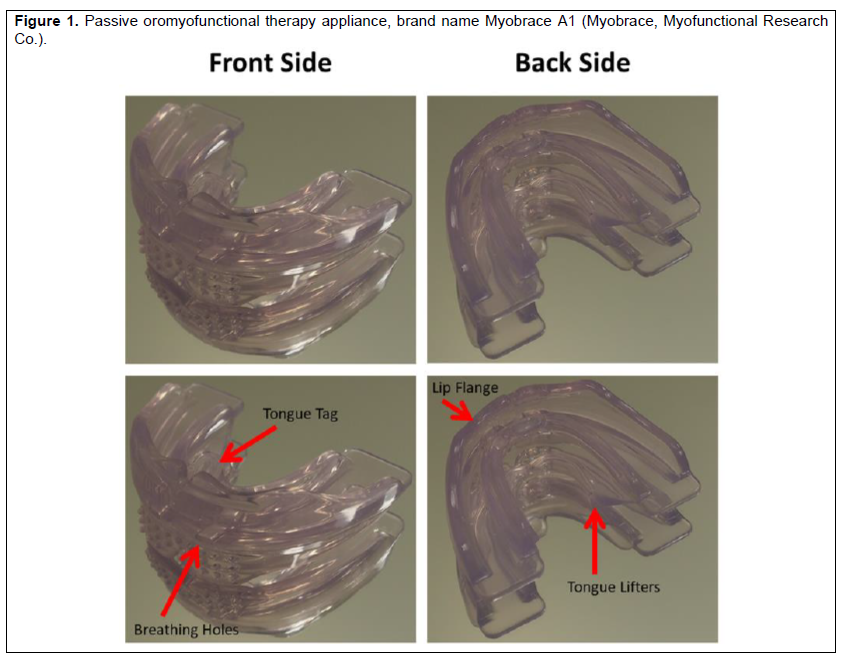
After discussions on the details pertaining to OAT, including its risks and benefits, the patient elected to proceed with OAT. However, the patient had some concern regarding the wait time related to manufacturing and appliance delivery, which was estimated at 4 weeks, and inquired about other treatment options during the wait period. Details pertaining to passive OMT appliances (Figure 1), their limitations, and American Academy of Sleep Medicine and American Academy of Dental Sleep Medicine practice guidelines were discussed. Specifically reviewed and emphasized was that passive OMT appliances are not titratable and are tissue borne, though they do possess components that encourage appropriate tongue positioning and lip seal. Also reviewed and emphasized was that passive OMT appliances are not recommended as a replacement for custom-fit titratable appliances for OAT. The patient elected to trial a passive OMT appliance during the wait period for her custom-fit titratable dental sleep appliance. Review of the clinical records indicated that the patient would be a potential responder to OAT with minimal protrusion with a vertical range of 3 to 7 mm, and that the patient had no contraindications for OAT. Based on data collected during the clinical examination, an appropriately sized passive OMT appliance (Myobrace A1, Myofunctional Research Co., Rancho Cucamonga, CA) to hold the appropriate mandibular position was provided to the patient to trial. The patient was aware that this was not considered a standard treatment but wanted to trial the passive OMT appliance. Because of the nature of this trial, the patient stated she understood the associated risks and agreed to follow up in the event of experiencing any adverse effects.
RESULTS
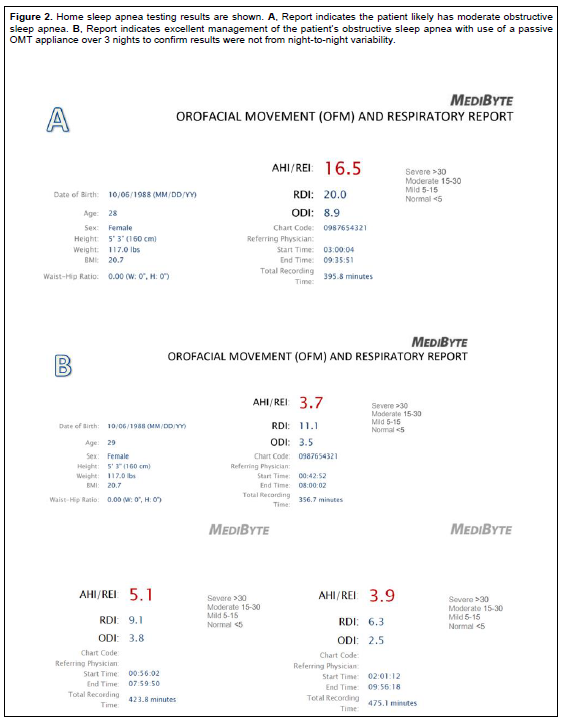
A home sleep study unit of the same type as the one used for the original diagnosis of the patient’s OSA (Figure 2, A) by the sleep physician was dispensed on the same day that the passive OMT appliance was provided. Instructions for use included wear of the appliance at nighttime only, rinsing the appliance with water prior to insertion and after removal from the mouth, and storing the appliance in a dry container or on a dry surface. Results showed the passive OMT appliance provided excellent management of the patient’s OSA (Figure 2, B). Because of the unexpected results of the study and to verify that the results were not due to night-to-night variability, an additional 2-night sleep study using the same unit was conducted, with both additional nights confirming excellent management of the patient’s OSA (Figure 2, B). The patient also reported immediate improvements to her sleep quality, decreased daytime sleepiness, improved vitality, and that her household reported no longer hearing her snoring. Over the following weeks, the patient also noted minimal difficulties with use of the passive OMT appliance, comfortable fit, and ability to maintain the appliance in the mouth through the entire night. The patient noted some limitations, however, such as an inability to speak when wearing the appliance, increased salivation, and the need to hide the appliance from her pets. Overall, the patient reported satisfaction with the passive OMT appliance and elected not to proceed with more traditional OAT.
Figure 1Passive oromyofunctional therapy appliance, brand name Myobrace A1 (Myobrace, Myofunctional Research Co.). |
{kind=link}
Figure 2Home sleep apnea testing results are shown. A, Report indicates the patient likely has moderate obstructive sleep apnea. B, Report indicates excellent management of the patient’s obstructive sleep apnea with use of a passive OMT appliance over 3 nights to confirm results were not from night-to-night variability.(more ...) |
{kind=link}
DISCUSSION
The use of passive OMT appliances in OAT for the treatment of SDB opens new possibilities for quick and immediate treatment for appropriately selected patients. Current American Academy of Sleep Medicine and American Academy of Dental Sleep Medicine practice guidelines indicate that only custom-fit, titratable appliances should be used in the treatment of SDB. This is likely because of previous research indicating significant mandibular protrusion was indicated for OAT.5,6 However, newer research has shown that minimal mandibular protrusion may be sufficient in OAT.7 These techniques used for mandibular positioning may allow for appropriate selection of passive OMT appliances to be an acceptable alternative to more traditional appliances for OAT. The nonprotrusive nature of passive OMT appliances may decrease the risks of adverse effects commonly associated with traditional protrusion techniques used in OAT.7-10 Furthermore, passive OMT appliances may also include components for appropriate tongue positioning, which may aid in mitigating the tongue collapsing into the airway during sleep. Further research into the use of passive OMT appliances and specific and appropriate patient selection criteria for their use in OAT is necessary.
Other than the inherent limitations in any case study, other limitations in this clinical case include the use of HSAT rather than overnight monitored polysomnography and not using multinight studies to help account for night-to-night variability in sleep testing. Annual follow-up sleep testing to confirm maintenance was also not yet available.
CONCLUSION
This case report shows the successful use of a passive OMT appliance for OAT in the treatment of a patient with moderate OSA, reducing the patient’s apnea-hypopnea index from 16.5 to 3.7 and resolving the patient’s chief concerns related to sleep quality and daytime sleepiness. Further research and testing in the possible use of passive OMT appliances for other patients with OSA should be explored.
ACKNOWLEDGEMENTS
The authors would like to thank Dr. Manuel Lagravere for his mentoring and aid in the preparation of this manuscript.
ABBREVIATIONS
Continuous positive airway pressure: CPAP
Home sleep apnea test: HSAT
Obstructive sleep apnea: OSA
Oral appliance therapy: OAT
Orofacial myofunctional disorders: OMDs
Orofacial myofunctional therapy: OMT
Sleep breathing disorders: SBDs
Upper airway resistance syndrome: UARS
REFERENCES
- de Felício CM, da Silva Dias FV, Folha GA, et al. Orofacial motor functions in pediatric obstructive sleep apnea and implications for myofunctional therapy. Int J Pediatr Otorhinolaryngol. 2016;90:5-11. doi: 10.1016/j.ijporl.2016.08.019..
- Guilleminault C, Huang YS, Monteyrol PJ, Sato R, Quo S, Lin CH. Critical role of myofascial reeducation in pediatric sleep-disordered breathing. Sleep Med. 2013;14(6):518-525. doi: 10.1016/j.sleep.2013.01.013.
- Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: a systematic review and meta-analysis. Sleep. 2015;38(5):669-675. doi: 10.5665/sleep.4652.
- de Felício CM, da Silva Dias FV, Trawitzki LVV. Obstructive sleep apnea: focus on myofunctional therapy. Nat Sci Sleep. 2018:10:271-286. doi: 10.2147/NSS.S141132..
- Piskin B, Karakoc O, Genc H, et al. Effects of varying mandibular protrusion and degrees of vertical opening on upper airway dimensions in apneic dentate subjects. J Orofac Orthop. 2015;76(1):51-65. doi: 10.1007/s00056-014-0259-z.
- Aarab G, Lobbezoo F, Hamburger HL, Naeije M. Effects of an oral appliance with different mandibular protrusion positions at a constant vertical dimension on obstructive sleep apnea. Clin Oral Investig. 2010;14(3):339-345. doi: 10.1007/s00784-009-0298-9.
- Ng ET, Mayoral P, Hernandez IA, Lagravere MO. Comparing anterior protrusive with sibilant phoneme mandibular positioning techniques for dental sleep appliances in managing obstructive sleep apnea: a retrospective study. J Dent Sleep Med. 2021;8(1).
- Pliska BT, Nam H, Chen H, Lowe AA, Almeida FR. Obstructive sleep apnea and mandibular advancement splints: Occlusal effects and progression of changes associated with a decade of treatment. J Clin Sleep Med. 2014;10(12):1285-1291. doi: 10.5664/jcsm.4278.
- Perez CV, de Leeuw R, Okeson JP, et al. The incidence and prevalence of temporomandibular disorders and posterior open bite in patients receiving mandibular advancement device therapy for obstructive sleep apnea. Sleep Breath. 2013;17(1):323-332. doi: 10.1007/s11325-012-0695-1.
- Sheats R, Schell T, Blanton A, et al. Management of side effects of oral appliance therapy for sleep-disordered breathing. J Dent Sleep Med. 2017;04:111-125. doi: 10.15331/jdsm.6746.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication November 9, 2021
Submitted in final revised form February 15, 2022
Accepted for publication November 13, 2022
Address correspondence to: Dr. Enoch Ng, Clinical Dentist, Enjoy Dental, Edmonton, Alberta, Canada. Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta Canada, T6G 1C9; Email: enoch@ualberta.ca