Case Report 1, Issue 10.1
Combined Oral Appliance Therapy and Adjunctive Minimally Invasive Er:YAG Laser Therapy for Complete Resolution of Severe Obstructive Sleep Apnea: A Clinical Case Report
http://dx.doi.org/10.15331/jdsm.7280Marcela Bisheimer, DDS, MSc, PhD1; Enoch T. Ng DDS2; Manuel O. Lagravere, DDS, MSc, PhD2; Pedro Mayoral, DDS, MSc, PhD1
1University Católica de Murcia UCAM, Faculty of Medicine and Dentistry, School of Dentistry, Madrid, Spain; 2School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alberta, Canada
ABSTRACT
This case report describes the use of laser therapy from an Er:YAG laser in conjunction with a custom-fit titratable dental sleep appliance for the resolution of a patient’s severe obstructive sleep apnea, daytime sleepiness, snoring, and breathing sounds when sleeping.
Keywords:
laser, dentistry, sleep appliance, obstructive sleep apnea
Citation:
Bisheimer M, Ng ET, Lagravere MO, Mayoral P. Combined oral appliance therapy and adjunctive minimally invasive Er:YAG laser therapy for complete resolution of severe obstructive sleep apnea: A clinical case report. J Dent Sleep Med. 2022;10(1)
INTRODUCTION
Obstructive sleep apnea (OSA) is a type of sleep breathing disorder that affects from 9% to 38% of the population.1-3 OSA occurs when the upper airway in the oropharynx collapses during sleep, resulting in difficulties with breathing during sleep. OSA is well associated with other medical conditions, including diabetes and cardiovascular disease. Depending on its severity, OSA is most frequently treated with positive airway pressure (PAP) machines, dental sleep appliances, positional therapy, and weight loss.
Over the past few years, nonsurgical laser therapy for snoring has gained popularity within medicine and dentistry. As early as 2011, dentists were using erbium-doped yttrium aluminium garnet lasers (Er:YAG) in a nonsurgical manner to decrease snoring to improve patient quality of life.4 The use of nonsurgical lasers for treating snoring has become very popular, with two lasers dominating the market: the Lightwalker AT-S by Fotona (specific protocol for snoring: Nightlase) and the Solea by Convergent (specific laser protocol for snoring: Solea Sleep).5,6 However, as of 2020, research still showed that although nonsurgical laser therapy was able to significantly decrease snoring, it is not an effective treatment for OSA.7
This case report will demonstrate the use of combining a dental sleep appliance with nonsurgical laser therapy to manage a patient’s severe OSA, without the required use of the dental sleep appliance for maintenance of the resolution. One-year follow-up will show sustained complete resolution of the patient’s OSA.
REPORT OF CASE
A 71-year-old woman presented to a multidisciplinary sleep center with primary concerns of loud snoring with observed apneas. The patient’s medical history was significant for vascular stenosis and bilateral cataracts, for which she had undergone phakectomy (cataract surgery). The patient reported no allergies and currently not taking any medications. Clinical assessment of the patient noted a height of 161 cm, weight of 57 kg, and body mass index of 22 kg/m2. The patient scored 9 on the Epworth Sleepiness Scale, 4 on the STOP-BANG assessment, and 9 on a visual analog scale of 0 to 10 for snoring volume. Review of disturbed sleep symptoms with the patient revealed self-reported loud, continuous snoring that worsened over the past 5 years, observed apneas by a bedpartner, poor sleep quality, unrefreshing sleep, difficulty with waking up in the mornings, and tiredness throughout the day. The patient noted she did not experience dry mouth, headaches, or nocturia (having to wake up to go to the bathroom). Based on this initial assessment, a home sleep apnea test (BTI APNiA, Biotechnology Institute, Vitoria, Spain) was provided to the patient with instructions for appropriate wear and use.
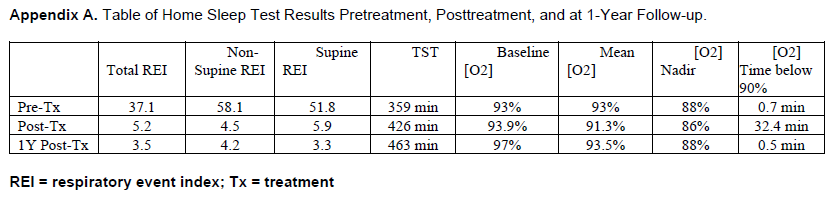
The sleep test results were scored and reviewed by a sleep physician, who then made the diagnosis of severe OSA in the patient. The patient’s respiratory event index (REI) was 37.1, though a postural component was noted as the supine REI was 51.8. The average oxygen saturation recorded throughout the night was 93%, with the lowest oxygen saturation during the study night of 88%. A table of sleep study results is presented in Appendix A. The patient returned to the multidisciplinary sleep center to review the results after which the sleep physician discussed and reviewed appropriate treatment options with the patient. Because of the severity of the patient’s OSA, the first line of treatment recommended to the patient was PAP therapy. However, the patient was not interested in PAP therapy and requested other treatment options. After review with a multidisciplinary team on other treatment options including a custom-fit dental sleep appliance, laser therapy, a combination of both, and surgical options, the patient opted for combined dental sleep appliance with laser therapy.
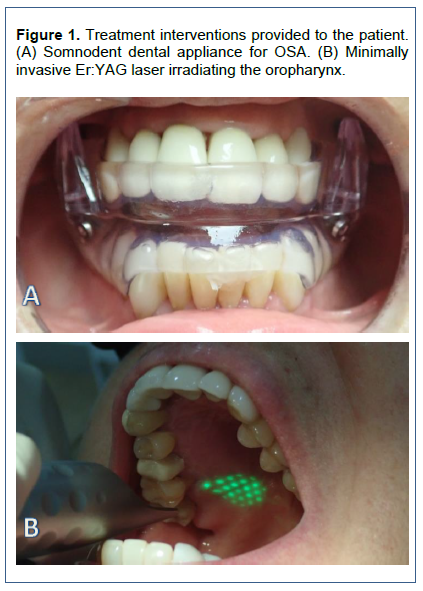
A custom-fit dental appliance (SomnoDent, Barcelona, Spain) was provided to the patient at a dental sleep medicine clinic with an initial mandibular position set at 50% of maximum mandibular protrusion. (Figure 1.) The patient was shown how to appropriately insert and remove the appliance, then demonstrated her ability to do so before leaving her appointment. Appropriate home care instructions for the use and maintenance of the appliance were reviewed and also provided to the patient in writing. The patient was shown the SnoreLab app, which she downloaded onto her phone, and was instructed to use it to record her snoring volume while sleeping, with the purpose being to objectively monitor her snoring for comparison before, during, and after treatment.
The first laser therapy session was provided 2 months later at an outpatient laser clinic. The patient’s oropharynx was irradiated with an Er:YAG laser (Lightwalker AT-S, Fotona) under settings previously described by Monteiro et al8 (Figure 1).
“The patients were all treated… with a 2940nm wavelength Er:YAG laser (Lightwalker AT-S, Fotona®, Slovenia) with a non-contact irradiation of connective and muscle tissue of oropharynx (soft palate including uvula, anterior and posterior pillar’s, and rest of oropharynx) using a PS04 handpiece with 7-mm spot size. The parameters were set as a combination of a long pulse (LP0 with a fluence of 2J/cm2 with 12Hz in a brushing technique with 6 passes in a well-defined overlays and a smooth mode with a fluence of 10-8J/cm2 with 2Hz performing 4-6 smooth pulses with 6 passes, with an overlap around 50%, with total pulses ranging between 10,000 and 12,000 pulses per sessions. Usual safety precautions related with the instrument for protecting the operator, patient, and assistant were followed.” (e562) 8
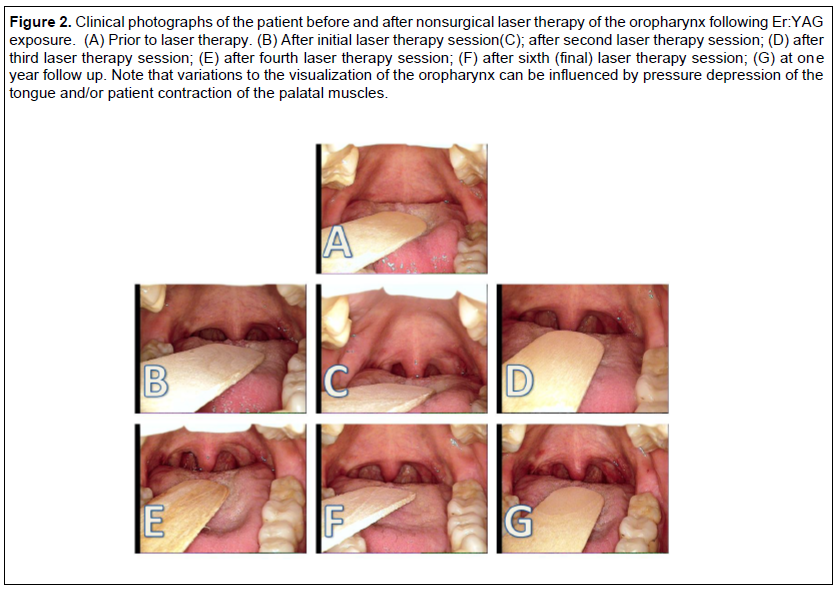
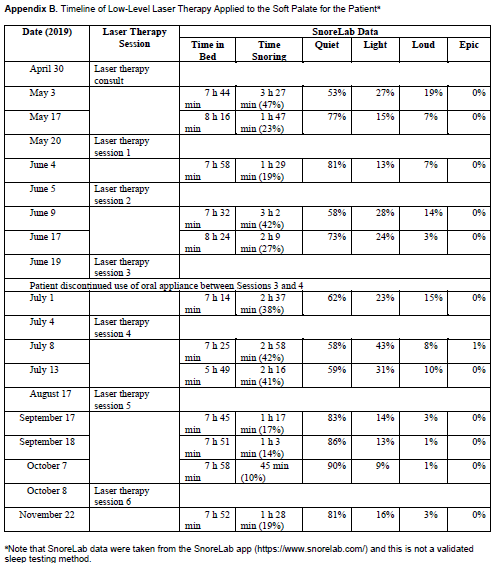
The patient reported no ill effects and no discomfort during the procedure. The patient was then scheduled for three additional laser therapy sessions set apart biweekly, then an additional two sessions 3 months apart. A table outlining the dates of the laser therapy sessions is presented in Appendix B. The patient was also scheduled for her 1- year sleep study follow-up. Clinical photos were taken of the patient’s oropharynx before the initial laser therapy and after each laser therapy session (Figure 2). The patient was instructed to continue to use her dental appliance, and the SnoreLab results were also recorded at each session. The results indicated that the patient’s snoring volume was decreasing.
After the third laser session, the patient discontinued use of her dental sleep appliance. Her stated reasons were due to improved symptoms and no longer wanting to wear the appliance. Even after discussions with the dental and sleep physician members of the multidisciplinary sleep team, the patient continued to refuse to wear her dental sleep appliance but wanted to continue with the laser therapy. The decision was made to continue to provide the laser therapy portion of her treatment and to re-evaluate her via a follow-up sleep study as originally scheduled. At her annual follow-up, the patient was provided with the follow-up sleep study as scheduled to evaluate the management of her severe OSA. The results of the sleep study, without a dental sleep appliance, were as follows: REI, 5.2; supine REI, 5.9. (Appendix A)
One year later the patient underwent standard annual follow-up with a sleep study to confirm appropriately maintained management of her OSA. The results of the sleep study included an REI of 3.5 and a supine REI of 4.2 (Appendix A). Review of the patient’s medical history revealed no reported changes to weight, sleep position, general medical status, medications, or any other medical interventions since the patient’s last sleep study at her last visit.
Figure 1Treatment interventions provided to the patient. (A) Somnodent dental appliance for OSA. (B) Minimally invasive Er:YAG laser irradiating the oropharynx. |
{kind=link}
Figure 2Clinical photographs of the patient before and after nonsurgical laser therapy of the oropharynx following Er:YAG exposure. (A) Prior to laser therapy. (B) After initial laser therapy session(C); after second laser therapy session; (D) after third laser therapy session; (E) after fourth laser therapy session; (F) after sixth (final) laser therapy session; (G) at one year follow up. Note that variations to the visualization of the oropharynx can be influenced by pressure depression of the tongue and/or patient contraction of the palatal muscles. |
{kind=link}
Appendix ATable of Home Sleep Test Results Pretreatment, Posttreatment, and at 1-Year Follow-up. |
{kind=link}
Appendix BTimeline of Low-Level Laser Therapy Applied to the Soft Palate for the Patienta |
{kind=link}
DISCUSSION
Currently, the first-line treatment for severe OSA is the use of PAP machines. Although these have been shown to be efficacious, there are significant difficulties with the use of PAP machines in terms of comfort and compliance for patients, with long-term use of PAPs significantly lacking. For this reason, the use of custom-fit dental sleep appliances are also considered an effective treatment due to greater patient compliance when compared to use of PAPs. However, though patient compliance and comfort are improved with dental sleep appliances, adverse effects (such as facial pain/soreness and occlusal/bite changes) are still common and can be problematic with long-term use.
Nonsurgical laser therapy has been used in multiple fields for the treatment of different diseases and conditions including wound healing, scar reduction, nerve injuries, to improve cognitive function and decrease inflammation in patients with chronic pain. More recently, nonsurgical laser therapy has also gained popularity within medicine and dentistry for the treatment of snoring, though there has still been little research to show its effectiveness in the treatment of OSA.7-11 However, interest in the use of lasers for the treatment of snoring and eventually for sleep breathing disorders is growing.
This case report shows that the combined use of a dental sleep appliance with nonsurgical laser therapy may be considered a treatment option for patients with severe OSA. Although a dental sleep appliance may be used for initial immediate management, it can be speculated that laser therapy appropriately applied at the oropharynx over multiple sessions may help with improving oropharyngeal patency. Over time, this may result in the maintenance of oropharyngeal patency without the continued need for a dental sleep appliance. This would eliminate the risks associated with long-term use of dental sleep appliances and any compliance concerns surrounding the use of the appliance while still providing complete therapeutic benefit in the treatment of patients with severe OSA.
CONCLUSION
This case report shows the successful combined use of nonsurgical laser therapy with the transitional use of a dental sleep appliance for the resolution of severe OSA in a single patient. Further research into this combination of treatment through efficacy studies as well as through blinded randomized controlled trials with placebo control groups with long-term sleep testing and clinical photography documentation of the oropharynx to assess changes to pharyngeal tissues are necessary to determine the generalizability of this therapy modality and the development of appropriate patient selection criteria for its use.
REFERENCES
- Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311-1322. doi:10.3978/j.issn.2072-1439.2015.06.11
- Benjafield AV, Ayas NT, Eastwood PR, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Respir Med. 2019;7(8):687-698. doi:10.1016/S2213-2600(19)30198-5
- Lyons MM, Bhatt NY, Pack AI, Magalang UJ. Global burden of sleep-disordered breathing and its implications. Respirology. 2020;25(7):690-702. doi:10.1111/resp.13838
- Kakkar M, Malik S, Gupta B, Vaid N, George R, Singh S. Use of Laser in Sleep Disorders: A review on low laser uvulopalatoplasty. Sleep Disord. 2021;2021:8821073. Published 2021 Feb 28. doi:10.1155/2021/8821073
- Martinez K. A simple and non-surgical solution for snoring. https://www.dentalproductsreport.com/view/simple-and-non-surgical-solution-snoring. Updated 2020. Accessed July 6, 2021.
- Shiffman HS. How to use breakthrough nonsurgical laser sleep applications. https://www.dentalproductsreport.com/view/how-to-use-breakthrough-nonsurgical-laser-sleep-applications. Updated 2020. Accessed July 6, 2021.
- Neruntarat C, Khuancharee K, Shoowit P. Er:YAG laser for snoring: A systemic review and meta-analysis. Lasers Med Sci. 2020;35(6):1231-1238. doi: 10.1007/s10103-020-02987-3.
- Monteiro L, Macedo A, Corte-Real L, Salazar F, Pacheco JJ. Treatment of snoring disorder with a non-ablactive er:YAG laser dual mode protocol. An interventional study. J Clin Exp Dent. 2020;12(6):e561-e567. doi: 10.4317/jced.56953.
- Cetinkaya EA, Turker M, Kiraz K, Gulkesen HK. Er:Yag laser treatment of simple snorers in an outpatient setting. ORL J Otorhinolaryngol Relat Spec. 2016;78(2):70-76. doi: 10.1159/000443510.
- Frelich H, cierski W, Marków M, Frelich J, Frelich H, Maciej M. Minimally invasive erbium laser treatment for selected snorers. Lasers Med Sci. 2019;34(7):1413-1420. doi: 10.1007/s10103-019-02731-6.
- Storchi IF, Parker S, Bovis F, Benedicenti S, Amaroli A. Outpatient erbium:YAG (2940 nm) laser treatment for snoring: A prospective study on 40 patients. Lasers Med Sci. 2018;33(2):399-406. Accessed 11 April 2020. doi: 10.1007/s10103-018-2436-6.
SUBMISSION & CORRESPONDENCE INFORMATION
Submitted for publication November 9, 2021
Submitted in final revised form February 15, 2022
Accepted for publication November 13, 2022
Address correspondence to: Dr. Enoch Ng, DDS, Graduate Student, School of Dentistry, Faculty of Medicine and Dentistry, University of Alberta, 11405 - 87th Avenue, Edmonton, Alberta Canada, T6G 1C9; Email: enoch@ualberta.ca